Download
1 / 99
990 likes | 1.27k Views
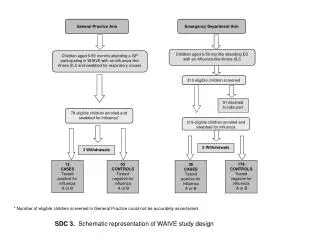
Emergency Department Safety Assessment and Follow-up Evaluation (ED-SAFE). Treatment as Usual Site Training. Outline of Presentation. Phase overview Inclusion/exclusion criteria Case identification and enrollment Forms. Outline of Presentation. Phase overview Inclusion/exclusion criteria

E N D
Emergency Department Safety Assessment and Follow-up Evaluation (ED-SAFE) Treatment as Usual Site Training
Outline of Presentation • Phase overview • Inclusion/exclusion criteria • Case identification and enrollment • Forms
Outline of Presentation • Phase overview • Inclusion/exclusion criteria • Case identification and enrollment • Forms
Data Collection Phases Treatment as Usual Screening Alone Intervention Phase Slide 4
Data Collection Phases In all phases: Patient enrollment in ED 5 follow-up phone calls In the Intervention Phase, subjects will receive additional telephone counseling Slide 5
Treatment as Usual Clinically, patients will be screened for self-harm and treated according to the usual care at the site We will use lessons learned from sites as we move into the next phases Slide 7
Treatment as Usual RAs will screen ED documentation (charts, electronic information systems) in “real time” to identify patients RAs will further screen anyone with evidence of any intentional self-harm ideation or behavior in the past week, including the current visit This will involve asking the clinicians for permission to approach the patient Slide 8
Treatment as Usual While clinical staff’s cooperation is vital, we do not want to introduce treatment contamination Emphasize that we don’t want clinical staff to do anything different than they ordinarily would The clinical staff should not be told to let the RAs know when a suicidal patient is present (i.e., referral) Slide 9
Outline of Presentation • Phase Overview • Inclusion/exclusion criteria • Case identification and enrollment • Forms
Inclusion Criteria Age ≥18 years Suicidal ideation or behavior in the past week, including current visit Able to consent (alert, fully oriented, not intoxicated, able to paraphrase the study requirements) Willing to complete telephone follow-up assessments at 6, 12, 24, 36, 52 weeks Slide 11
Exclusion Criteria Medically/cognitively unable to participate Currently dwelling in a non-community setting (e.g., acute psychiatric facility) Currently in state custody Pending legal action Lack of permanent residence Lack of reliable telephone service Insurmountable language barrier Already enrolled into ED-SAFE Slide 12
Outline of Presentation • Phase overview • Inclusion/exclusion criteria • Case identification and enrollment • Forms
Site Enrollment Goal 60 subjects 30 subjects with suicidal ideation only in past week 30 subjects with suicidal attempt in past week 60 / 50 weeks = 1.2 / week Slide 14
Case Identification RA will screen in “real time” all charts for ED patients ≥18 years old who are triaged during their shift Use the ED triage log (tracking system) to monitor patients triaged during shift Slide 15
ED Coverage 40 hours/week required Shift days and hours flexible Recommendations: coverage between noon and 10 pm one weekend day per month, minimum Target: screen ~50 charts/8-10 hr shift Slide 16
Case Identification (cont'd) Will need to order patients chronologically by triage time Start screening chart of the first patient triaged after the start of the RA’s shift RAs may approach patients with documented self-harm if the patient is present in the ED when the shift starts even if the patient was triaged prior to the start of the RA’s shift. Slide 17
Case Identification (cont'd) Screen all consecutive charts of patients ≥18 y.o. for any intentional self-harm thoughts or behaviors Approach patients who have documented self-harm thoughts/behaviors and who otherwise seem to meet eligibility criteria Slide 18
Case Identification (cont'd) If chart or MD clearly identifies stable exclusion criteria, such as mental retardation, brain damage, homelessness, or insurmountable language barrier, then the patient does not have to be approached Slide 19
Case Identification (cont'd) If chart or MD identifies transient exclusion criteria (e.g., intoxication) the patient should be “pending” or “warm” and approached later Pending patients should be “resolved” at the end of every shift Stable exclusion criteria Left ED before RA approach End of RA shift Slide 20
Eligibility If deemed “approachable,” RA completes the eligibility screening interview at the bedside If eligible, RA initiates consent process Should emphasize the importance of the study in helping us to understand how to better help people who are suicidal Should be a thorough discussion of responsibilities Allow patient a little time to think about it Slide 21
Eligibility Some may be eligible and interested, but the time may not be opportune (e.g., too distracted to participate during ED visit, busy with tests, being transferred to inpatient setting) May consent admitted or “boarded” patient within 48 hours of ED discharge “Warm” transfer Slide 22
04/15/10 Slide 23
Enrollment After consent, patient should be enrolled Locator form – in ED Baseline assessment – in ED Chart review – after ED visit Utilization Summary – after ED visit Healthcare Utilization Forms – after ED visit Slide 24
Follow-up Assessments 6 and 12 months Utilization Summary Healthcare Utilization Form(s) Vital Statistics Form Slide 25
Outline of Presentation • Phase overview • Inclusion/exclusion criteria • Case identification and enrollment • Forms
Forms Recommendation during shift: • Paper-based Screening Log • REDCap (computer-based) forms for all other enrollment tasks (eligibility screening, locator form, baseline assessment)
Screening Log All charts screened in “real time” should be documented on the paper Screening Log during the shift All Screening Log data must be entered at least weekly into REDCap Shift screening summary Screening log ID #s automatically assigned in each database Slide 29
Screening Log (cont'd) Completeness of Screening Log (paper and REDCap) is a crucial part of the entire data collection process Helps RA to keep track of people in “real time” (paper) Will provide information for describing the representativeness of the sample and reasons for exclusion Will provide information for Quality Assurance efforts Slide 30
Screening Log (cont'd) Review all documentation available in the ED At minimum, review the triage nursing notes Stop the review once you identify any self-harm and approach the patient When possible, review charts in order, but do not miss people with SI/SA. Screening ID # automatically assigned in REDCap; not necessary to include on paper version Slide 31
Screening Log (cont'd) Data collected include: Shift start time, end time RA initials Order of presentation Triage time Age Sex Ethnicity and race Presence of self-harm thoughts or behavior Whether or not the patient was approached Name, MRN, bed – for site RA use only Slide 32
Screening Log (cont'd) Screening Log Order of Presentation Patient’s Chart Reviewed Answer “no” if there was no chart available for review (e.g., pt registered and “in the system,” but left before any triage notes documented) or ED became too busy for you to keep up with screening Stop screening Self-harm Thoughts or behaviors Suicidal or non-suicidal Slide 33
Ethnicity and Race On Screening Log, record as it is documented in the chart / administrative databases Two distinct concepts, but some hospital systems treat them as the same Example 1 “Race” documented as Hispanic Record ethnicity as Hispanic; race as not documented Slide 34
Ethnicity and Race (cont'd) Example 2 Race documented as Puerto Rican Record ethnicity as Hispanic; race as not documented Example 3 Ethnicity and race both documented as Hispanic Record ethnicity as Hispanic; race as not documented Example 4 Documentation on the chart reads “white male” Record ethnicity as not documented; race as white * See the MOP for definitions Slide 35
Screening Log (cont'd) Requires Follow-up Use to flag patients that require follow-up the next day For patients admitted with evidence of SI or SA with a potentially transient state that kept them from being enrolled in the ED (e.g., intoxication) Patient Approached Continue to Eligibility Screening Slide 36
Screening Log (cont'd) Quality Assurance Regular review of REDCap by EMNet staff to compare against estimates/projections Cross-validation of screening logs against ED logs in a random sample of 5% of enrollment days Helps to ensure that the consecutive screening nature of the protocol is being applied with fidelity to avoid selection bias Slide 37
Eligibility All potentially eligible patients should be entered in real time into the REDCap Screening Log Enter the eligibility screening questions in the REDCap Screening Log Slide 38
Screening Log (cont'd) Shift Screening Summary Shift Date Shift Start Time Shift End Time Slide 39
Eligibility Considerations Ask to speak one-on-one with the patient if others are in the room Ask about self-harm and suicidal behavior even if the patient does not report self-harm or suicidal ideation Slide 40
Eligibility Screening Assesses the following items: Self-harm and suicidal behavior and ideation If no suicidal behavior or ideation Characteristics that facilitate follow-up Phone always in service Wiling to participate in follow-up calls Permanent address and plan to stay there for 12 months If “no” to any of these characteristics Slide 41
Eligibility Screening (cont'd) Self-harm and suicidal behavior and ideation Thoughts of self-harm in past week Thoughts of ending life in past week Tried to hurt self in past week Tried to kill self in past week Slide 42
Wallet Card All patients approached – regardless of whether or not they are enrolled – receive a wallet card with a national hotline phone # Slide 43
Patient Resources Give all patients who decline to participate or meet exclusion criteria site-specific resources used by the ED for patients with psychiatric issues For example: a list with local mental health providers and services Slide 44
Consent Forms Separate consent for each phase Use color coded paper to easily identify TAU: Light blue Screening Alone: Light yellow Intervention: Light green Received a Certificate of Confidentiality (as stated on consent forms) Slide 45
Enrollment If an individual consents: 2 data collection “forms” need to be completed in the ED Locator form Baseline assessment Must record Subject ID # in the Screening Log. Slide 46
Subject ID# Each enrolled subject will have a unique Subject ID# Assign a 6-digit ID#: First 3 digits will be your site # Second 3 digits will be the consecutive # assigned to each subject No dashes Subject ID # is only for enrolled subjects Important: record Subject ID # on the eligibility “form” (i.e., enter it into the REDCap Screening Log) Slide 47
Locator Form Complete the Locator Form before the baseline assessment Record the subject’s preferred language (English or Spanish) Very important for all subjects to provide alternate contacts Emergency contact Non-cohabiting contact Slide 48
Locator Form (cont'd) However, subjects who are unable or unwilling to provide alternate contacts may still participate if they have a stable telephone and address Slide 49
Locator Form (cont'd) Ensure the subject has a working phone: After interview, call the subject’s primary number to confirm that it rings If phone not in service, re-approach the patient and fix the problem If the problem cannot be resolved, the subject cannot continue (protocol violation; report by filling out questions at end of baseline assessment) Slide 50