Download
1 / 19
260 likes | 526 Views
Health Risk Management. Today’s Presentation. Define Health Risk Management (HRM) Our vision The bottom line impact of poor Health Risk Management The scope of a proactive HRM study Elements Program Partnerships Long term study strategy Our enrollment progress to date.

E N D
Today’s Presentation • Define Health Risk Management (HRM) • Our vision • The bottom line impact of poor Health Risk Management • The scope of a proactive HRM study • Elements • Program • Partnerships • Long term study strategy • Our enrollment progress to date
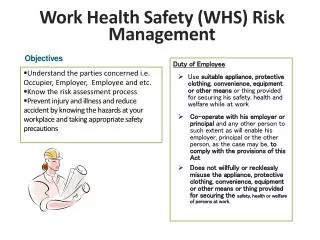
Health Risk Management • A worksite-based proactive approach to helping identify and reduce specific health risk factors through healthier lifestyle choices. • Assessment • Coaching and education • Specific interventions • Reporting
Our Vision • To reduce workers’ compensation costs and provide measurable benefits to policyholders by improving employee health and productivity. • Core areas of opportunity • Workers’ compensation cost and trend improvements • Increased productivity for employers • Improved health and wellness status of employees • Be a leader in the application of health risk management in workers’ compensation
Why Health Risk Management Now? Workplace Safety MedicalManagement OrganizationalCulture/Structure Health RiskManagement 1970s 1980s 1990s 2010 Employer Behavior Operational Behavior Employee Behavior
The Bottom Line Impact of Poor Health Risk Management • Workers’ Compensation Costs • Productivity • Health Insurance Claims
Medical 22% Disability 4% Total Cost of Poor Employee Health Workers’ Compensation Health Care Costs Medical Care Hospitalization Pharmacy Diagnostic Testing Behavior Health Physical Therapy Indemnity Costs Medical Costs DIRECT Sick Leave Other Wage Replacement Adverse Bottom Line Impact Lost Productivity Presenteeism Absenteeism Turnover Temporary Staffing Productivity Missed Deadlines Replacement Training OTHER COSTS Loss 74% Overtime Pay Sub Par Quality Employee & Customer Dissatisfaction
Workers’ Compensation: Direct Cost • A greater than 8-fold difference in w.c. costs between recommended weight and obese workers.Duke University • A 7-fold difference in w.c. costs between high and low risk workers.University of Michigan • A 23% decline over 2 years in w.c. claims costs and 18% decline in w.c. claims volume among companies engaging in HRM.Wellsource Health Solutions • Health risks have a compounding impact on w.c. costs • Obese claims are 2.8 times more expensive than non-obese claims at the 12-month maturity. The cost difference climbs to a factor of 4.5 at the three year maturity and to 5.3 at the five year maturity. National Council on Compensation Insurance (NCCI), 2009
Duke Study The most obese have 13 times more lost workdays than healthy weight workers 200 14 183.63 180 11.65 10.80 12 160 140 10 8.81 120 117.61 7.05 8 Claims per 100 FTEs Lost Workdays per 100 FTEs 100 5.80 5.53 75.21 6 80 60.17 60 4 40.97 40 2 14.19 20 0 0 BMI<18.5 (Underweight) 18.5 – 24.9 (Healthy Weight) 25 – 29.9 (Overweight) 30 - 34.9 (Obese Class I) 35 – 39.9 (Obese Class II) 40+ (Obese Class III) Lost Workdays Claims Source: Ostbye, T., et al, “Obesity and Workers Compensation,” Archives of Internal Medicine, April 23, 2007.
Duke Study Indemnity costs are 11 times higher for the most obese workers than for healthy weight workers. $70,000 $59,178 $51,091 $60,000 $50,000 $40,000 $34,293 $23,633 $23,373 $30,000 $19,661 $13,338 $13,569 $20,000 $7,109 $7,503 $5,396 $3,924 $10,000 $0 BMI<18.5 (Underweight) 18.5 – 24.9 (Healthy Weight) 25 – 29.9 (Overweight) 30 - 34.9 (Obese Class I) 35 – 39.9 (Obese Class II) 40+ (Obese Class III) Medical Claims Costs Indemnity Claims Costs Source: Ostbye, T., et al, “Obesity and Workers Compensation, ” Archives of Internal Medicine, April 23, 2007.
Productivity • Employers, on average, have $3 of health-related productivity costs for every $1 of medical or pharmacy claims costs. (Journalof Occupational & Environmental Medicine July 2007) • Lost productivity represents 7.9% of total corporate earnings and 5.3% of human capital costs. (Health and Human Capital Foundation) • The most costly conditions related to productivity are often not the same as the most costly conditions related to medical treatment costs. Taking an integrated approach to health and productivity results in more cost-effective interventions. (Journal of Occupational & Environmental Medicine July 2007)
Look Beyond Health Insurance Costs Back/Neck Pain Depression Fatigue Other Chronic Pain Sleeping Problem High Cholesterol Arthritis Hypertension Obesity Anxiety $0 $100,000 $200,000 $300,000 $400,000 $500,000 $600,000 Medical Drug Absenteeism Presenteeism JOEM July 2007
Impact of Health Insurance • The vast majority of Pinnacol policyholders have fewer than 25 employees • We assume the rate of uninsured status, from a health care perspective, mirrors the state as a whole • Approximately 50% of our participants are likely to have no health insurance • Placing HRM in a worksite environment rather than a health insurance environment is a key differentiator
We Believe In the future, Health Risk Management will be as fundamental to managing risk as safety is now.
Pinnacol HRM Components • 3-5 year timeframe • Partnering with key agencies • Free HRM services to policyholders • 3,000 participating policyholders representative of Colorado’s workforce (Small and medium sizes of employers are a critical component) • 30,000 enrolled members
Pinnacol’s HRM Program • Health Risk Assessment for employees • Health education and coaching • Specific interventions and programs • Reporting on participation and outcomes • Policyholders • Agents • Pinnacol • Colorado/national
Pinnacol’s HRM Partnerships Service Delivery - Interventions Wellsource Health Solutions (WHS) Reporting WHS: Health risk profile Integrated Benefits Institute: HPQ-Select Productivity Survey (Harvard-WHO tool) Data/Evaluation IBI, Thomson Reuters/Emory University/local universities
HRM Study Strategy • Use outside independent evaluators to conduct a peer review quality assessment of the long term impact of HRM on: • Health risk profile of our policyholders and their employees (based on trended HRA results) • Monetized changes in productivity (based on trended results of HPQ-Select) • Changes in Workers’ Compensation (based on participant pool versus Pinnacol control group) • Changes measured over 3 – 5 years • Work with local universities and researchers to identify other relevant issues and make data available for non-Pinnacol initiatives
Progress Toward our Study Goals Enrolled Policyholders Enrolled Employees 9,148 of 30,000 105 of 3,000 Data as of 8/27/2010