Download

1 / 49
490 likes | 660 Views
Collaborating to Finance Behavioral Health Services for Children and Their Families. SAMHSA/CMS Conference on Medicaid and Mental Health Services and Substance Abuse Treatment Arlington, VA September 2006 Beth Stroul, M. Ed . Frank Rider, MS Denise Baker. Literature Review.

E N D
Collaborating to Finance Behavioral Health Services for Children and Their Families SAMHSA/CMS Conference on Medicaid and Mental Health Services and Substance Abuse Treatment Arlington, VA September 2006 Beth Stroul, M. Ed. Frank Rider, MS Denise Baker
Literature Review Fragmented Funding • Funding sources for children's mental health services include a complex patchwork of funding streams across multiple systems • Financing of children’s behavioral health services is irrational, fragmented, categorical, and inflexible • Often does not support a full array of home and community-based services and supports • Disproportionate share resources are spent on residential and inpatient treatment • Results in cost shifting across systems
Literature Review Medicaid Funding • Over the past 15 years, states have increasingly relied on Medicaid to pay for health and mental health services • Medicaid budgets have escalated in states • Managed care technologies have been applied in most state’s Medicaid systems • Medicaid plays a key role in financing children’s mental health systems of care
Literature Review Effective Medicaid Financing Strategies: • Collaborative strategies for Medicaid dollars • Redirect spending from "deep-end" restrictive placements to home and community-based services and supports • Incorporate strong utilization and cost management mechanisms and systematically track costs • Incorporate case rate and risk adjustment strategies if operating within risk-based environments • Use behavioral health carve outs
Study of Effective Financing Strategies for Systems of Care Goals • Develop better understanding of critical financing structures and strategies to support effective systems of care • Examine how these financing strategies operate separately, collectively, and in the context of states and communities • Promote improved financing policies through dissemination of study findings and TA to states and communities
Study Hypotheses Effective Financing Strategies: • Identify Current Spending and Utilization Patterns Across Systems Determine utilization and costs Identify types and amounts of funding for behavioral services • Realign Funding Streams Utilize diverse funding streams Maximize the flexibility of state and/or local funding streams Coordinate cross-system funding Maximize federal entitlement funding (Medicaid, SCHIP, IV-E) Redirect spending from "deep-end" restrictive placements to home and community-based services and supports Financing to support a locus of accountability for managing care and costs for high-need populations Finance services to uninsured and underinsured children
Study Hypotheses • Finance an Appropriate Array of Services and Supports • Support a broad service array • Promote individualized, flexible service delivery • Support and provide incentives for the provision of evidence-based and promising practices • Promote and support early identification and intervention and early childhood mental health services • Support cross-agency service coordination/care management • Support Family and Youth Partnerships • Support family and youth involvement in policy-making • Support family and youth involvement and choice in service planning and delivery • Support services and supports to families/caregivers
Study Hypotheses • Financing to Improve Cultural/Linguistic Competence and Reduce Disparities in Care • Support culturally and linguistically competent services • Reduce racial/ethnic disparities in access • Reduce geographic disparities in access • Financing to Improve the Workforce and Provider Network • Support a broad, diversified, qualified workforce and provider network • Provide adequate provider payment rates
Study Hypotheses • Financing for Accountability • Incorporate utilization, quality, and cost management mechanisms • Utilize performance-based or outcomes-based contracting • Evaluate financing policies to ensure that they support and promote system of care goals and continuous quality improvement • Support leadership, policy, and management infrastructure for systems of care
Study Methods Participatory Action Research Approach • Continuous dialogue with key users on study methods Multiple Case Study Design • 10 site visits and 5 additional sites for telephone interviews • Panel of national financing experts nominated potential sites for the study • Sites demonstrate effective financing strategies in multiple domains • Sites demonstrate commitment to system of care philosophy and approach
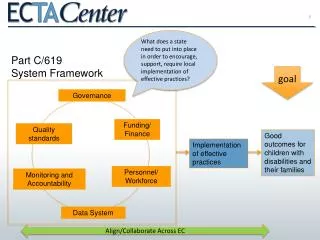
Critical Financing Areas • Identification of Current Spending and Utilization Patterns Across Systems for Strategic Planning • Realignment of Funding Streams and Structures • Financing of Appropriate Services and Supports • Financing to Support Family and Youth Partnerships • Financing to Improve Cultural/Linguistic Competence and Reduce Disparities in Care • Financing to Improve the Workforce and Provider Networks for Behavioral Health Services for Children and Families • Financing for Accountability
Selected Sites Selected Sites for First Wave of Site Visits • Maricopa County, Arizona • State of Vermont • Bethel, Alaska • State of Hawaii • Central Nebraska Telephone Interviews • Milwaukee Wraparound, Wisconsin • Dawn Project, Indianapolis, Indiana • State of New Jersey
Site Visits • Site visits involve interviews with key informants • Use of semi-structured interview protocol • Explore the implementation of critical financing strategies and challenges in each area
Products • Self-assessment and planning guide for state and community policymakers and planners to develop a comprehensive financing plan • Financing TA briefs with “how-to” information and examples from the site visits • Technical assistance to states and localities by partners
A Self-Assessment and Planning Guide:Developing a Comprehensive Financing Plan to Support Effective Systems of Care A Technical Assistance Tool for States, Communities, and Tribes
Purpose of Self-Assessment and Planning Guide • To assist states, communities, and tribes to: • Assess their current financing structures and strategies • Identify outcomes to achieve • Consider a variety of financing strategies • Prepare to develop a strategic financing plan • Not designed to provide detailed “how to” information for each strategy • Products with “how to” information will follow site visits
Areas Addressed in the Guide • Identification of Current Spending and Utilization Patterns Across Systems • Realignment of Funding Streams and Structures • Financing of Appropriate Services and Supports • Financing to Support Family and Youth Partnerships • Financing to Improve Cultural/Linguistic Competence and Reduce Disparities • Financing to Improve the Workforce and Provider Network • Financing for Accountability • Glossary • Links to Other Resources
How to Use the Guide • Deciding Where to Begin • What key stakeholders feel should be done first • Which strategies are in place and which need to be developed • Which strategies would provide short-term “wins” and which are longer-range • Which areas of guide would be most useful now • Selecting Outcomes • Reviewing and Selecting Strategies
Example – Realigning Funding Streams • Outcome • Increased proportion of funding used for home and community-based services in relation to funding for more restrictive services • Potential Strategies to Consider • Medicaid home and community-based waivers • Redirection of funds from bed closures and reduction in residential placements to community-based services and supports • Offer therapeutic foster care as alternative • Offer TEFRA as Medicaid option • Direct new monies to home and community-based services
Example – Realigning Funding Streams • More Strategies: • Define medical necessity and level of care criteria to allow for diversion from inpatient and residential care • Include residential providers in discussions about funding issues in moving to a community-based system • Provide TA and training to residential providers for developing home and community-based services and short-term psychiatric stabilization • Involve families in identifying the community-based services and supports that are needed and in advocating for the shift from residential to home and community-based services • Select Strategies and Develop Implementation Plan
Anticipated Outcomes of Financing Study • Revise and finalize set of critical financing strategies • Increased knowledge about and attention to critical financing strategies on the part of key stakeholders involved in building systems of care • Increased use of strategic financing plans for systems of care
FUND SOURCE FY 2006 FUNDS TOTAL FY 2006 FUNDS Children’s Percent of Children’s $ Medicaid/Title XIX (67.4% federal) $760,640,800 $269,079,100 88.68% SCHIP/Title XXI (77.185% federal) $15,130,000 $15,130,000 4.99% Federal Grants $44,631,300 $10,981,200 3.62% County Funds (Maricopa, Pima) $39,161,500 $1,803,000 0.59% State Appropriations $117,516,600 $6,444,600 2.12% $3,778,200 0 0.00% $980,858,400 $303,438,500 100.00% Other Total Funding Arizona BH Funding for Children
Arizona Financing Features • Pre-paid capitation (per member, per month) • Service planning process that engages positive contribution of families • Service planning process that attracts informal supports • Broad array of service/support options • Minimal prior authorization • Risk-adjusted capitation for children in state custody • Flexible funds
The Arizona Vision “In collaboration with the child and family and others, Arizona will provide accessible behavioral health services designed to aid children to: • achieve success in school • live with their families • avoid delinquency • become stable and productive adults Services will be tailored to the child and family and provided in the most appropriate setting, in a timely fashion, and in accordance with best practices, while respecting the child’s and family’s cultural heritage.” J.K. vs. Eden et al. No. CIV 91-261 TUC JMR, Paragraph 18
The 12 Arizona Principles • Collaboration with the Child and Family • Functional Outcomes • Collaboration with Others • Accessible Services • Best Practices • Most Appropriate Setting • Timeliness • Services Tailored to the Child and Family • Stability • Respect for the Child and Family’s Unique Cultural Heritage • Independence • Connection to Natural Supports
Principle: Collaboration with the Child and Family • Families mobilized to participate in collaborative workgroups (in the settlement process phase of JK litigation) • Maricopa Co. RBHA hired parent as a Systems Development leader (JK 300 Kids Pilot) • Arizona Children’s Executive Committee established Family Involvement Subcommittee • Policy established to compensate family members for their expertise • White paper written defining scope and nature of family involvement • Framework embraced by all Arizona child-serving agencies “Family Involvement Framework”adopted by Arizona Children’s Executive Committee
Importance of Family-Run Organizations • Mental health care is consumer and family drivenThe President’s New Freedom Commission Goal #2 • Family-Run Organizations as Transformation Agents Gary Blau, SAMHSA/CMHS – Federation of Families for Children’s Mental Health Conference 2005 • “Market Research”/Participatory Action Research What the customer needs, and how they want it • Persistent commitment to long-term change process • Provide wide array of enhancement to public system transformation efforts • Statewide Family Networks (47 states) • Arizona’s Family-Run Organization Partnership: MIKID and Family Involvement Center
Families Organize in Arizona • Shared Commitment among Key Partners: Families, State, RBHAs, Community • Example: St. Luke's Health Initiative (foundation) provided pilot funding: • Stipends • Consultative Resources • Training and Outreach
Covered BH Services in AZ • Prevention Services • Rehabilitation Services • Support Services • Treatment Services • Medical Services • Behavioral Health Day Programs • Crisis Intervention Services • Inpatient Services • Residential Services
Support Services Case Management Family Support Peer Support Respite Care Transportation Rehabilitation Services Living Skills Training Health Promotion Service Coding, FFS ratesdesigned tosupport community-based service delivery (Reference ADHS Covered BH Services Guide at: http://www.azdhs.gov/bhs/bhs_gde.pdf) Delivered by Professional, BH Technician, Para-professionals New Types of Provider Community Service Agency [CSA] Therapeutic Foster Care [TFC] Habilitation New Focus on Support and Rehabilitation Services
Child and Family Team Process • “The Child and Family Team is a group of people that includes, at a minimum, the child, the child’s family, any foster parents, a behavioral health representative and any individuals important in the child’s life who are identified and invited to participate by the child and family.” 1. Engagement 6. Plan Development 2. Immediate Crisis Stabilization 7. Plan Implementation 3. Strengths, Needs and Culture 8. Crisis Planning Discovery 4. Team Formation 9. Tracking and Adapting 5. Team Facilitation 10. Transition From ADHS Practice Improvement Protocol #7: “The Child and Family Team”
Child and Family Team (CFT) Process Based on the Wraparound Approach: Service planning is family-centered, strength-based, highly individualized, culturally competent and collaborative across systems, promoting reliance on informal and natural supports in combination with formal supports and services. Congruent with: • Family-Group Decision-Making (Child Welfare) • Team Decision-Making (Child Welfare) • Person-Centered Planning (Development Disabilities) • Individual Family Service Planning (IDEA - Part C)
Clinical Guidance Documents • Operationalize Principles • Memorialize Expectations • Developed through Collaborative Processes • “Guidance” Contractual Requirements Examples: Child and Family Team PIP and TAD Reference: http://www.azdhs.gov/bhs/guidance/guidance.htm
Families Join the Behavioral Health Workforce • Family Support Partners • Work alongside case managers and clinicians to ensure effective family voice within Child and Family Teams • Today over 70 family members are employed in provider agencies • Juvenile Justice: Parent Liaisons (early implementation) • Child Welfare: Parent Mentors (role being developed) • Provision of Direct Family-to-Family Services • Family Support (Home Care Training) • Peer Support • Peer Support Group • Skills Training • Skills Training Group • Behavioral Health Promotion Education & Training • Respite
Benefits of Family Support as a Behavioral Health Service • Prepares families to benefit from clinical services • Increases value of clinical services • Leverages cost-effective natural supports • Enhances workforce with skilled, committed members: • para-professional, technical skills complement professional services • Well-trained, experienced personnel (family organization/CSA or OBHL-licensed clinic) • Workforce that resembles the people we serve • Mitigates nationally-strained BH workforce limitations
Therapeutic Foster Care:A Programming Success Story • Family-Based Alternative to Congregate Care • Braiding Medicaid and Title IV-E Resources • ADHS Practice Improvement Protocols: • Therapeutic Foster Care Services for Children • Out of Home Care Services • Recruitment, Licensing and Certification • PS-MAPP and TFC Advanced Curriculum • TFC Capacity Growth: • September 2003 – 9 placements statewide • September 2006 – 404 placements (40% of all OOH)
Family Partnership with MCO’s:Wide Array of Key Roles within Arizona’s Family-Driven System of Care • Involvement in recruitment, hiring, creating job descriptions, shaping supervision guidelines • Development of practice protocols • (Co-)Trainers for BH workforce • Consultative resources • Continuous Quality Improvement roles (example: Arizona CFT process measurement)
Quality Management Processes CFT Process Measurement’s Four Big Questions: • Has a trusting relationship been established with the family (engagement)? • Does the Child and Family know the family and has it identified the strengths needs and culture of the family? • Has an Individualized Service Plan been created that meets the needs of the child and family? • Is the team implementing, monitoring and modifying the service plan toward a successful outcome for the child and family?
Fall 2005 Reviews Region A – 67.8% Region B – 64.1% Region C – 74.1% Region D – 66.3% Region E – 73.3% Region F – 41.7% Statewide: 53.25% [n = 486] Winter 2006 Reviews Region A – 70% Region B – 64% Region C – 71% Region D – 61% Region E – 81% Region F – 53% Statewide: 60.45% [n = 418] Quality Management:CFT Process Measurement
Wraparound Milwaukee: Residential placements decreased by 60% Psychiatric hospitalization decreased by 80% Reduced recidivism by delinquent youth Decreased overall cost of care per child Bruce Kamradt, Child Welfare League of America, 2001 National Conference; and Report of the Surgeon General on Children’s Mental Health (1999) Project MATCH/Pima County AZ: High fidelity CFT practice connected to significantly better outcomes than low fidelity CFT practice on standardized measures: Child/Adolescent Functioning [CAFAS] Child Behavior Checklist [CBLC] Restrictiveness of Living Environment Scale [ROLES] Family Resource Scale [FRS] Rast, O’Day, Bruns & Rider, 17th Annual Research Conference in Children’s Mental Health (2004) (n = 63 CFTs, fidelity per WFI 2.1, -6 to +12 months) Improved Processes Improved Outcomes
Outcomes for Arizona Childrenwith/without Child and Family Teams (5-11 y.o.)
Outcomes for Arizona Youthwith/without Child and Family Teams (12-17 y.o.)
Participatory Action Research Approach [PAR] Participatory action research = collective, self-reflective enquiry undertaken by participants in social situations in order to improve the rationality and justice of social practices. Kemmis and McTaggart (1988) The four components of action research are: 1. Observation 2. Reflection 3. Planning 4. Action How Arizona families participate in PAR: • Session Rating Scales (Family to Family services) • Outcome Assessment (within CFT process) • CFT Process Measurement • JK Annual Planning Process • JK Committee
A Few Last Words… • Medicaid Administrators -Families have much to offer: • expertise about what works and what doesn’t work • can work in partnership with treatment professionals to provide necessary and cost-effective services • Mental Health/Substance Abuse Administrators - • Consumers and families are a traditionally untapped sources of expertise about effective service delivery approaches • Resources (e.g. funding) must be designated to leverage their transformational voices • Avoid tokenism – prepare, support families as you do all other experts • Family Members - • Be part of the solution (“non-adversarial advocacy”) • Organize to ensure a family-driven system of care
For further information: Denise Baker, Parent/Consultant c/o The Family Involvement Center, Phoenix AZ bake423@orbitelcom.com Frank Rider MS, Director Arizona Institute for Family Involvement frank@familyinvolvementcenter.org Beth Stroul M.Ed., Vice President Mgmt. & Training Innovations Inc., McLean VA bethstroul@aol.com