Download
1 / 47
470 likes | 638 Views
Osteochondroses of the Foot. TONY PASCOE B.App.Sc. (Pod) Grad.Dip.(Pod) M.A.Pod.A. OSTEOCHONDROSES. Group of bone disorders in the growing skeleton in which the centres of ossification undergo aseptic necrosis, followed by bone resorption, and then repair

E N D
Osteochondroses of the Foot TONY PASCOE B.App.Sc. (Pod) Grad.Dip.(Pod) M.A.Pod.A
OSTEOCHONDROSES • Group of bone disorders in the growing skeleton in which the centres of ossification undergo aseptic necrosis, followed by bone resorption, and then repair • Primary pathology is a vascular deficit in the subchondral region of the involved bone
Osteochondritis • Osteochondritis juvenilis • Aseptic necrosis • Avascular necrosis • Infarction • Osteonecrosis
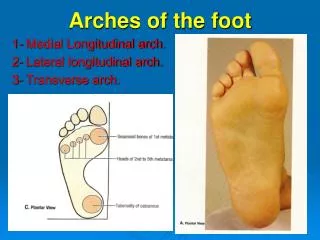
More Common • Sever’s Disease (heel) • Kohler’s Disease (navicular) • Iselin’s Disease (5th metatarsal) • Freiberg’s Disease (2nd metatarsal) Less Common • Diaz or Mouchet’s Disease (talus) • Buschke’s Disease (cuneiforms) • Treves’ or Ilfelds’Disease (sesamoids) • Thiemann’s Disease (phalanges)
Sever’s Disease (Osteochondrosis of Calcaneal Apophysis) First described in 1912 by J.W Sever MD in New York Medical Journal Described as an “inflammation of the calcaneal apophysis resulting in pain at the posterior heel, mild swelling and difficulty walking”
Sever’s Disease PATHOPHYSIOLOGY • Calcaneal apophysis develops as an independent centre of ossification in boys aged 9-10 years and fuses by age 17 (girls slightly younger age) • Apophyseal line appears weakened during rapid growth (puberty) because of increased fragile cartilage • Microfractures believed to occur because of shear stress leading to normal progression of fracture healing
Sever’s Disease PATHOPHYSIOLOGY • Radiographic appearance of resorption, fragmentation and increased sclerosis leading to eventual union • BUT…… Xrays showing fragmentation of apophysis are NOT diagnostic, as multiple centres of ossification may exist in normal apophysis
Sever’s DiseaseINCIDENCE No exact figures/data Higher in boys than girls Occurs most frequently between ages of 8-15 years Peak incidence around 10-11 years
Sever’s DiseaseAETIOLOGY Decreased resistance to shear stress at bone-growth plate interface Research indicates traction apophyses have a higher composition of fibrocartilage than epiphyses subjected to more axial load, composed predominantly of hyaline cartilage Traction from tight Achilles tendon
Sever’s DiseaseDIFFERENTIAL’S Stress fracture Tumour Tarsal Coalition Insertional Achilles Tendinopathy Osteomyelitis
Sever’s DiseaseTREATMENT R.I.C.E Heel raise Triceps surae stretching program Correct Footwear Foot Orthoses if required Complete immobilisation rarely required
Sever’s DiseaseWHEN TO REFER TO SURGEON NEVER ………. Unless suspect tumour, coalition or infection
KOHLER’S DISEASE AVN of navicular bone occurring spontaneously or as a result of trauma during ossification process Onset at 4yrs (3-5 yrs female, 4-5 yrs male) Less than 1/3 are bilateral More common in boys
Kohler’s DiseaseSIGNS AND SYMPTOMS • Pain at navicular • Increased perfusion • Aversion to footwear • Antalgic gait • Flattening and narrowing of navicular on plain xray
Kohler’s Disease Sclerosis, irregularity and early collapse of the navicular consistant with avascular necrosis (Kohler’s disease)
Kohler’s DiseasePROPOSED PATHOLOGY Largely speculative, but 3 main theories: • Mechanical: repetitive, compressive forces • Physiological: ossification irregularities are not uncommon and more often seen in later developing bones • Co-morbidities: malignancies, chemotherapy and radiation can cause ossification delays
Kohler’s DiseaseTREATMENT • Rest: As a self limiting disease, normal function will resume within 24 months (avg 18mths) • Orthoses: reduction in compressive force to encourage renewed vascularisation • Immobilisation (BK Cast or CAM walker for at least 8 weeks)
ISELIN’S DISEASE • Traction apophysitis of tuberosity of 5th metatarsal • Occurs at attachment of peroneusbrevis • More common than generally appreciated
TIMELINES • Occurs in older active children or young adolescents • Coincides with appearance of the proximal apophysis of tuberosity of 5th metatarsal • Apophysis appears in females at age 9.7 yrs and males 12.1 years, and fuses with shaft of 5th met by age 11 yrs in females and 14 years in males
(ISELIN’S DISEASE) SYMPTOMS • Tenderness over a prominent proximal 5th metatarsal • Pain over lateral aspect of foot with weightbearing • More common with lateral movement sports which cause inversion stress on forefoot
(ISELIN’S DISEASE) CLINICAL EXAM FINDINGS • Larger 5th met tuberosity • Localised soft tissue swelling and mild erythema • Tender at insertion of peroneus brevis • Pain with resisted eversion, plantarflexion and dorsiflexion
(ISELIN’S DISEASE) DIFFERENTIALS • Avulsion fracture • Jones fracture • Os Vesalianum • Peroneal tendinopathy
(ISELIN’S DISEASE) TREATMENT • R.I.C.E • Foot orthoses with lateral wedging/posting • Footwear choices • Cross training
FREIBERG’S DISEASE • First described by Freiberg in 1914 as an infarction of the 2nd metatarsal head • Can affect the head of any lesser metatarsal, 2nd most common (70%) • Onset 11-17 yrs of age (F>M)
Freiberg’s disease AETIOLOGY • No consensus • Classed as an osteochondrosis, but this does not explain the adult onset of the disease?? • Most likely multifactorial cause, with initial insult primarily vascular or traumatic (?biomechanical influence)
Freiberg’s Disease CLINICAL PRESENTATION • Initially asymptomatic, but later pain on walking • Local tenderness and limp • Limited joint ROM with pain on direct palpation of metatarsal head • Possible periarticular oedema and soft tissue swelling
Freiberg’s Disease DIFFERENTIALS • Stress fracture • Morton’s neuroma • Synovitis • Plantar plate injury • Gout
Freiberg’s Disease X-RAY CLASSIFICATION • Fracture of subchondral epiphysis • Flattening of articular surface with early collapse of central protion of metatarsal • Further flattening and collapse of central protion with medial and lateral projections
Freiberg’s Disease X-RAY CLASSIFICATION • Loose bodies form and lateral projections break off • End stage arthrosis
Freiberg’s Disease Early Stage 1
Freiberg’s Disease Stage 2 - 3
Freiberg’s Disease Stage 4
Freiberg’s Disease Stage 5
Freiberg’s Disease TREATMENT • Accommodative padding to relieve pressure • Metatarsal bar/pad • Orthoses • BK casting • Surgical – excision of fragments, metatarsal head removal, joint implants
DIAZ OR MOUCHET’S DISEASE • Very rare • Associated with acute trauma with compression of talar dome • Usually remodels to normal shape
BUSCHKE’S DISEASE • Very rare • Effects each of the cuneiforms • Pain in region of cuneiforms • Affected cuneiform has irregular outline on xray
TREVES’ OR ILFELD’S DISEASE • Significant pain on dorsiflexion and palpation of sesamoids • F>M • Fragmentation of sesamoid on xray • Need to distinguish from multipartite sesamoid or fracture