Download
1 / 39
810 likes | 1.15k Views
The Heart Outcomes Prevention Evaluation (HOPE) – 3 Trial. Eva Lonn, Jackie Bosch, Salim Yusuf For the HOPE-3 Investigators Population Health Research Institute, McMaster University and Hamilton Health Sciences, Hamilton, Canada. Disclosures. Eva Lonn

E N D
The Heart Outcomes Prevention Evaluation (HOPE) – 3 Trial Eva Lonn, Jackie Bosch, Salim Yusuf For the HOPE-3 Investigators Population Health Research Institute, McMaster University and Hamilton Health Sciences, Hamilton, Canada
Disclosures • Eva Lonn • Institutional Research Grants/ Contracts: Astra Zeneca, CIHR, Amgen, Bayer, GSK, Merck Shering, Eli Lilly, Sanofi • Consulting/ Lectures fees: Amgen, Cadila Pharmaceuticals, Novartis, Sanofi, Servier • Jackie Bosch • Institutional Research Grants/ Contracts: Astra Zeneca, CIHR, Cadila Pharmaceuticals, Bayer, Boehringer-Ingelheim, Novartis • Consulting Fees: Bristol-Myers Squibb • Salim Yusuf • Institutional Research Grants/ Contarcts: Astra Zeneca, CIHR, Cadila Pharmaceuticals, Bayer, Boehringer-Ingelheim, Bristol-Myers Squibb, Novartis • Consulting/Lecture fees and Travel Expenses: Bayer
Study Rationale • Graded increase in CVD risk for SBP >115 mmHg & for LDL throughout documented ranges in populations • BP lowering trials indicate reductions in CVD in high risk people and those with SBP>150 -160 mmHg • Statins lower CVD in secondary prevention and in primary prevention mainly in Whites with increased LDL-C or CRP, diabetes, or hypertension
Study Objectives To evaluate in an intermediate risk population without CVD the effects on CV events of: • BP lowering with combined Candesartan 16 mg + HCTZ 12.5 mg daily • Cholesterol lowering with Rosuvastatin 10 mg daily • Combined BP and cholesterol lowering
Intermediate-Risk Population • No strict BP or LDL-C criteria for entry • Uncertainty principle
The HOPE-3 Trial Global Trial: 228 centers in 21 countries Argentina, Australia, Brazil, Canada, China, Colombia, Czech Republic, Ecuador, Hungary, India, Israel, Korea, Malaysia, Netherlands, Philippines, Russia, Slovakia, South Africa, Sweden, United Kingdom, Ukraine
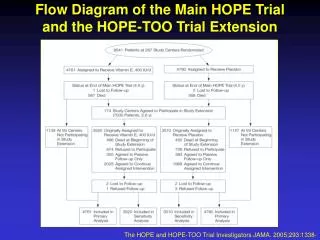
HOPE-3: 2 by 2 Factorial Design 14,682 Entered Single-blind 4 week Active Run-in 12,705 (87%) Randomized Candesartan 16 mg + HCTZ 12.5 mg n= 6,356 Placebo n = 6,349 Rosuvastatin 10 mg n=6,361 Rosuvastatin Cand+HCTZ n = 3,180 Rosuvastatin n = 3,181 Placebo n = 6,344 Cand+HCTZ n = 3,176 Double Placebo n = 3,168 Simple follow-up and few blood tests
Adherence and Follow-up • Median Follow up: 5.6 years • Participant Follow-up: 99.1% • High adherence
Outcomes • Co-Primary 1 • Composite of CV death, MI, stroke (p<0.04) • Co-Primary 2 • Composite 1 + resuscitated cardiac arrest, heart failure, revascularizations (p<0.02) • Secondary Outcomes • Composite of Co-Primary 2 + angina with objective ischemia • Stroke
Pre-Specified Hypothesis Based Subgroup Analyses • According to thirds of baseline: • Systolic BP • LDL-C • INTERHEART Risk Score
BP Lowering vs. Placebo: SBP Changes 140 Placebo 135 130 Systolic Blood Pressure (mmHg) Candesartan/HCTZ 125 Δ BP=6.0/3.0 mmHg 120 0 1 2 3 4 5 6 7 Years Cand/HCTZ 6356 5907 5667 5446 5213 3862 1437 350 Placebo 6347 5879 5623 5442 5186 3822 1424 334
CV Death, MI, Stroke, Cardiac Arrest, Revascularization, Heart Failure 0.10 HR (95% CI) = 0.95 (0.81-1.11) 0.08 P-value = 0.51 0.06 Placebo Cumulative Hazard Rates 0.04 Candesartan+HCTZ 0.02 0.0 0 1 2 3 4 5 6 7 Years No. at Risk Cand + HCTZ 6356 6272 6200 6103 5968 4969 2076 522 Placebo 6349 6270 6198 6096 5967 4970 2075 488
Coronary Heart Disease HR (95% CI) = 0.83 (0.64-1.06) 0.04 Stroke P-value = 0.14 0.020 HR (95% CI) = 0.80 (0.59-1.08) 0.03 P-value = 0.14 0.015 Placebo Cumulative Hazard Rates Placebo 0.010 0.02 0.005 Candesartan+HCTZ Candesartan+HCTZ 0.01 0.0 0 1 2 3 4 5 6 7 Years 0.0 0 1 2 3 4 5 6 7 Years BP Lowering vs. Placebo Coronary Heart Disease: Fatal/non-fatal MI, Coronary Revascularization
Prespecified Subgroups: By Thirds of SBP CV Death, MI, Stroke SBP Mean Placebo Event Rate% Cutoffs Diff P Trend HR (95% CI) 2.9 122 ≤131.5 6.1 1.16 (0.82-1.63) 0.021 131.6-143.5 138 5.6 3.8 1.08 (0.80-1.46) 154 >143.5 6.5 5.8 0.73 (0.56-0.94) 0.5 1.0 2.0 Cand + HCTZ Better Placebo Better
Prespecified Subgroups: By Thirds of SBP CV Death, MI, Stroke, Cardiac Arrest, Revasc, HF SBP Mean P Trend HR (95% CI) Placebo Event Rate% 3.5 1.25 (0.92-1.70) 0.009 Cutoffs Diff 4.6 1.02 (0.77-1.34) 122 ≤131.5 6.1 7.5 0.76 (0.60-0.96) 131.6-143.5 138 5.6 154 >143.5 5.8 0.5 1.0 2.0 Candesartan + HCTZ Better Placebo Better
BP Lowering Arm: Conclusions • Fixed dose combination of Candesartan 16 mg + HCTZ 12.5 mg/day reduced BP by 6.0/3.0 mmHg, but did not reduce CV events • CV events were significantly reduced in the highest third of SBP: SBP >143.5 mmHg, mean 154 mmHg • Results were neutral in the middle third, and trended towards harm in the lowest third of SBP • Treatment increased lightheadedness, but not syncope or renal dysfunction
Cholesterol Lowering Arm Results J. Bosch
LDL-C(mg/dL) APO B-100 (g/L) 0.8 Placebo 130 1.1 0.7 120 1.0 0.6 110 0.9 0.5 100 0.4 0.8 90 Rosuvastatin 0.3 0.7 80 0 Year 1 Year 3 Study End 0 Year 1 Year 3 Study End 0 Year 1 Year 3 Study End CRP (log)(mg/L) Cholesterol Lowering Arm:Change in LDL, Apo-B, and CRP Placebo Placebo mean Δ 34.6 mg/dl* mean Δ 0.23 g/l* log mean Δ 0.19* Rosuvastatin Rosuvastatin * P< 0.001
CV Death, MI, Stroke, Cardiac Arrest, Revasc, Heart Failure 0.10 HR (95% CI) = 0.75 (0.64-0.88) P-value = 0.0004 0.08 Placebo 0.06 Cumulative Hazard Rates 0.04 Rosuvastatin 0.02 0.0 0 1 2 3 4 5 6 7 Years Rosuva 6361 6241 6039 2122 Placebo 6344 6192 5970 2073
0.020 0.04 Stroke Coronary Heart Disease HR (95% CI) = 0.74 (0.58-0.96) HR (95% CI) = 0.70 (0.52-0.95) P-value = 0.0227 P-value = 0.0214 0.015 0.03 Placebo Placebo 0.010 0.02 Rosuvastatin Rosuvastatin Cumulative Hazard Rates 0.005 0.01 0.0 0.0 0 1 2 3 4 5 6 7 0 1 2 3 4 5 6 7 Years Years Coronary Heart Disease: MI, Coronary revascularization
Cholesterol Lowering:Subgroups Co-Primary 2 % Events Placebo Hazard Ratio (95% CI) P Interaction* Overall 5.7 0.75 ( 0.64 - 0.88 ) LDL <=112 6.0 0.69 ( 0.52 - 0.92 ) LDL 112-141 6.0 % 0.75 ( 0.57 - 1.00 ) LDL >141 5.5 % 0.93 ( 0.71 - 1.22 ) 0.145 INTERHEART Risk Score Tertile 1 <=12 4.6 % 0.66 ( 0.49 - 0.89 ) Tertile 2 13-16 5.6 % 0.81 ( 0.61 - 1.07 ) Tertile 3 >16 7.2 % 0.77 ( 0.60 - 0.98 ) 0.486 CRP <=2.0 5.6 % 0.79 ( 0.62 - 0.99 ) CRP >2.0 6.1 % 0.78 ( 0.63 - 0.98 ) 0.992 SBP <=131.5 4.7 % 0.65 ( 0.47 - 0.88 ) SBP 131.6-143.5 5.2 % 0.79 ( 0.60 - 1.05 ) SBP >143.5 7.3 % 0.80 ( 0.63 - 1.01 ) 0.335 Ethnicity European descent 6.0 % 0.62 ( 0.43 - 0.89 ) Chinese 4.5 % 0.73 ( 0.52 - 1.02 ) Other Asian 6.3 % 0.82 ( 0.59 - 1.13 ) Latin American 5.9 % 0.82 ( 0.61 - 1.09 ) Other 10.3 % 0.76 ( 0.40 - 1.42 ) 0.790 *P for trend for LDL, Risk Score, and SBP 0.5 1.0 2.0 Rosuvastatin Better Placebo Better
Cholesterol Lowering: Conclusions • Rosuvastatin 10mg/day reduced: • LDL-C by 34.6 mg/dl (0.9 mmol/l; i.e. 26% in LDL-C) • CVD by 25% • Consistent benefits regardless of: • LDL-C • SBP • Risk • CRP • Ethnicity • No excess in rhabdomyolysis, myopathy or diabetes; excess in muscle pain/weakness (reversible) and cataracts surgery (requires confirmation)
Combined BP & Cholesterol Lowering vs Double Placebo Salim Yusuf
HOPE-3: 2 by 2 Factorial Design N = 12,705 Cand 16 mg+ HCTZ 12.5 mg n= 6,356 Placebo n = 6,349 Rosuva 10 mg n=6,361 Rosuva + Cand+HCTZ n = 3,180 Rosuvan = 3,181 Placebo n = 6,344 Cand+HCTZ n = 3,176 Double Placebo n = 3,168
140 Combination vs Double Placebo:Change in SBP and LDL-C Double placebo 135 Rosuva SBP Cand + HTCZ 130 Mean Δ 6.2 mmHg Combination 125 120 Week 6 0 Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Year 7 Month 6 Double Placebo Rosuva. 140 Cand+HCTZ Cand + HCTZ Combination 120 Double placebo LDL-C 100 Rosuva Mean Δ 33.7 mg/dl 90 Combination 80 0 Year 1 Year 3 Study End 232 232 232 232 Rosuvastatin 247 247 247 247 Candesartan/HCTZ 248 248 248 248 Double placebo
CV Death, MI, Stroke, Cardiac Arrest, Revasc, Heart Failure 0.10 Double Placebo Cand + HCTZ 0.08 Rosuvastatin Combination 0.06 Cumulative Hazard Rates 0.04 0.02 HR (95% CI) = 0.72 (0.57-0.89) P-value = 0.0030 0.0 0 1 2 3 4 5 6 7 Years Combination 3180 4 3063 1057 Rosuvastatin 3181 3061 1045 Candesartan/HCTZ 3176 3040 1019 Double Placebo 3168 3035 1030
Coronary Heart Disease Stroke 0.025 0.05 HR (95% CI) = 0.56 (0.36-0.87) HR (95% CI) = 0.62 (0.43-0.88) 0.020 P-value = 0.0094 0.04 P-value = 0.0085 0.015 0.03 0.010 0.02 Cumulative Hazard Rates 0.005 0.01 0.0 0.0 0 1 2 3 4 5 6 7 0 1 2 3 4 5 6 7 Years Years Candesartan/HCTZ only Double Placebo Rosuvastatin only Combination Coronary Heart Disease: Fatal/non-fatal MI, Coronary Revascularization
Lower Two SBP Thirds 50% 50% Overall 40% 40% 31% 28% 26% 30% 30% RRR 20% 20% 20% 6% 10% 10% Candesartan/HCTZ Only 0% 0% Combination Combination Rosuvastatin Only Rosuvastatin Only Cand + HCTZ Only -7% Benefits of Combination and Each Intervention vs. Double Placebo Highest SBP Third 50% 39% 40% 30% 21% RRR 18% 20% 10% 0% Rosuvastatin Only Combination Candesartan/HCTZ Only
Combination vs Double Placebo: Conclusions • About a 30% reduction in major vascular events • Benefits of combination therapy: • Largely seen in those in the upper third of SBP (40% RRR in CVD) • In lower two thirds the benefit is from Rosuvastatin only (30% RRR in CVD)
Clinical Implications • Statins beneficial in all participants • BP lowering benefits only those with elevated BP • Combination therapy: • In hypertensives, leads to a 40% risk reduction (benefits from both BP lowering and statin) • In others, 30% RRR from statin alone • Pragmatic strategy without: • Lipid or BP criteria • Dose titration • Frequent monitoring HOPE-3 strategy is simple, effective, safe and low cost, and is globally applicable
HOPE-3 Results Published today in the NEJM: • Lonn E, Bosch J, Lopez-Jaramillo P, et al., for the HOPE-3 Investigators. Blood pressure lowering in intermediate risk people without vascular disease. NEJM 2016. • Yusuf, S., Bosch, J., Dagenais, G., et al. for the HOPE-3 Investigators. Rosuvastatin in intermediate-risk people without cardiovascular disease. NEJM 2016. • Yusuf, S., Lonn, E., Pais, P. et al. for the HOPE-3 Investigators. Blood pressure and cholesterol lowering in people without cardiovascular disease. NEJM 2016.
Acknowledgements • We would like to thank: • The Steering Committee • The Data and Safety Monitoring Committee • The Investigators and Study Coordinators for all their efforts We are very appreciative of the efforts made by all participants!!