Download
1 / 33
400 likes | 900 Views
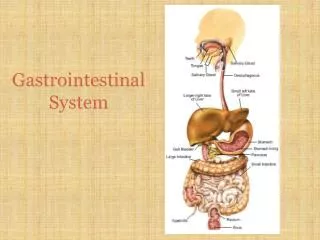
Gastrointestinal System. History & Examination with common OSCE examples for Finals. By Maryam Haneef, FY1 Medicine. History. Abdominal pain SOCRATES Peptic Ulcer disease : dull, burning, gnawing, epigastric , relief with food, episodic Cannot tell if GU or DU with just history!

E N D
Gastrointestinal System History & Examination with common OSCE examples for Finals By Maryam Haneef, FY1 Medicine
History • Abdominal pain SOCRATES • Peptic Ulcer disease: • dull, burning, gnawing, epigastric, relief with food, episodic • Cannot tell if GU or DU with just history! • Pancreatic: • Steady, epigastric, relief sitting forward, radiates to back, vomiting • Biliary: • Severe epigastric pain, episodic (biliary obstruction-’biliary colic’) • Shift to RUQ, more severe (cholecystitis) • Hepatic: • Dull ache, RUQ • Bowel: • Colicky • Periumbilical, frequent cycles of pain (small bowel) • Longer period between pain (colonic) • Vomiting, constipation, distension (obstruction)
ABDO PAIN (cont.) • Appendix • RIF pain, stabbing to dullache, started periumbilical? Guarding, rebound tenderness • Oesophagitis • Retrosternal discomfort/burning • “heartburn” • Travels up throat, after meals, bending/lying supine • “water brash” and sour taste in mouth • Worse: alcohol, chocolate, caffeine, fatty meals, anti-cholinergics, calcium channel blockers (reduce LOS tone)
Nausea and Vomiting • GI infection • Obstruction • Small bowel (volvulus, intersusseption) • Gastric outlet (PUD) • Pregnancy • Drugs • Opiates, digoxin, chemo • Gastroparesis • Diabetes mellitus, recent gastric surgery • Acute hepatobiliary disease • Biliary colic, cholecystitis, hepatitis • Pancreatitis
Vomitus • Coffee Ground • PUD • Bilious • Patent passage between stomach and duodenum • Blood streaked • Mallory-Weiss • Bleeding ulcer • Stomach Ca
Dysphagia • Rule out painful swallowing (ODYNOPHAGIA) • Infectious oesophagitis (candida, herpes) • Peptic ulcer of Oesophagus • Oesophageal perf. • Solids/liquids • Progressive deterioration solid to liquid: Stricture • Ca • Extrinsic pressure: retrosternal goitre, lung Ca • Oesophageal web, benign stricture • Difficult initiating swallow/regurgitation into nose/choking • Pharyngeal: neurological (MND, MG) • Food sticking • Point out where • Intermittent/initial swallows: Oesophageal spasm • Solids and liquids: Achalasia • Neck bulge/gurgling: pharyngeal pouch
Bleeding • Hameatemesis • Proximal to duodenum • Sx PUD? (could be acute peptic ulcer, no Hx pain) • Hx repeated vomiting/retching (Mallory-Weiss) • Acute setting: Large volume, pt unwell, Hx Liver disease (variceal bleed) • Others: gastric Ca, vascular anomolies • Melaena • Jet black stool • Bleed from upper GI tract (occasional small R-sided colonic or small bowel lesions) • Fresh PR bleed (Haematochezia) • On top of stool/in toilet bowl/on toilet paper • Haemorrhoids/anal fissures • Diverticular disease • Mixed with stool • Ulcerative colitis, colorectal Ca
Jaundice • Yellow discolouration: skin/sclera • Pale stools, dark urine, pruritis • Obstructive/cholestatic jaundice • Short duration, malaise, fever, anorexia • Viral hepatitis (recent travel, IVDU, sexual Hx) • Abdo pain • Episodic, colicky, RUQ : gallstones • Dull, persistent epigastric or central radiating to back: pancreatic Ca • Fever or rigors: cholecystitis/cholangitis • FH recurrent jaundice • Haemolytic anaemias, Gilbert’s
Diarrhoea • Defined as passing of >300g loose stool per day • Secretory • High volume, persists on fasting, no pus/blood, not fatty • Infection: E.coli, staph aureus, vibrio cholera • Hormonal: carcinoid, Zollinger-Ellison • Villous adenoma • Factitious diarrhoea: laxative abuse • Osmotic • Large volume, stops by fasting • Medication: lactulose, Mg antacid • Lactose intolerance • Gastric surgery
Diarrhoea (Cont.) • Abnormal intestinal motility • Thyrotoxicosis, IBS, Addison’s • Exudative • Inflammation in colon, small volume stool with blood/mucus • IBD, colon Ca • Malabsoprtion • Steatorrhoea: pale, fatty, v.smelly, floaters! • “more than 7g fat in 24-hour stool sample” • Chronic pancreatitis, bile salt deficiency (liver disease, extrahepatic obstruction), bacterial overgrowth, terminal ileal disease
Constipation • Infrequent passage of stool, hard stool, difficult to evacuate • Straining? anal block? self-digitate? • Recent change: obstructive ?Ca • Medication • Opiates, antidepressants (TCA’s), iron, aluminium/calcium antacids • Endocrine • Hypothyroidism, diabetes, • Pain • Fissure-in-ano, post-op, haemorrhoids • Lifestyle • Neglect impulse to defecate: accumulate hard stool, constant rectal distension thus lose awareness • Neuroligical • Disorder of pelvic floor muscle, hirschsprungs, autonomic neuropathy, spinal cord injury, multiple sclerosis • Slow transit
Other symptoms • Abdominal bloating/swelling • Excess gas • IBS • Persistent: Ascites • Lethargy • Acute/chronic liver disease • Anaemia: Ca, IBD, chronic GI disease
Complete History by: • PMH • Previous surgery to GI system • Previous GI problems • Transfusions • Dental treatment • DH • medication could be causing symptoms • SH • Occupation: exposure to toxins (carbon tetrachloride, vinyl chloride) causing liver disease, health care workers exposed to hepatitis • Travel Hx • Drug misuse • Alcohol Hx • Tattoos • FH • Colon Ca, IBD • Jaundice, anaemia, splenectomy, cholecystectomy
Finally... • Very brief relevant systems review • End History by: • Summarise and confirm • Ask pt concerns • Thank pt • Summarise findings: • “This is a X yr old lady/gent who presented with a Y day/week/month Hx of Z. Brief description of relevant findings. Based on this assessment my differentials are XYZ. Brief plan to investigate.” • Investigations: • Routine bloods: FBC, U+Es, LFTs, CRP, Clotting • Imaging: CXR/AXR, USS abdomen, ERCP/MRCP, CT, flexible sigmoidoscopy/colonoscopy, biopsy • Specific specialised tests: Liver screen, Coeliac screen, Hameatinics, H.pylori test, Ascitic tap
Examination • Wash hands • Introduction • Explanation • Very brief history: “what’s brought you in today? Where about is the pain?” • ABC!! • Just to let examiner know you know!
Inspection • At bedside: • well, comfortable, chachectic, sitting forward/very still, rolling in bed, drowsy/alert • obvious pallor or jaundice • SOB, tremulous • Obvious abdominal distension • Stoma • Surrounding: • Catheter • Ascitic drain • Oxygen • NG tube • Iv fluids
Inspection (cont) • Hands and nails • Clubbing: liver cirrhosis, IBD, Coeliacs, GI lymphoma • Palmer erythema • Dupuytren’s contracture • Leuchonychia: hypoalbuminaemia • cirrhosis, protein-losing enteropathy • Koilonychia • Asterixes/hepatic flap: encephalopathy • Bullae: porphyria cutanea tarda • Alcoholic liver disease
Inspection (cont.) • Arms: • Scratch marks • Obstructive jaundice, lymphoma • Bruising: hepatic impairment • Muscle wasting • Alcohol, steroid use, malignancy • Face: • Jaundice • Anaemia • pallor of conjunctiva, glossitis, angular stomatitis • Kayser-Fleischer rings: Wilson’s disease • Iritis: IBD • Xanthelasma: Primary Biliary Cirrhosis • Pigmentation of mucosa • Peutz-Jegher’s synd., chronic liver disease, Addison’s • Apthous ulcers and lip swelling: Chron’s Iritis Xanthelasma
Inspection...finally • Trunk • Spider naevi • >5 in SVC distribution: CLD, pregnancy, hyperthyroidism • Gynaecomastia: CLD • Sexual hair loss: CLD • Abdomen • Scars • distension: fluid, fat, flatus, faeces, fetus, fibroids • Caput medusae • Bruising • Cullen’s and Grey Turner’s : acute pancreatitis • Obvious peristalsis: obstruction/very thin • Legs • Pitting oedema
Palpation • Ask pt where is pain? (start away from here) • Follow quadrants/regions • Watch pt’s face throughout! • Masses • Site • Tenderness • Size • Surface/edge • Consistency • Mobility • Pulsatile? • Get above or below? • Guarding/rebound tenderness: peritonitis
Examination of Liver • Hand parallel to costal margin • RIF to costal margin • Feel on inspiration • Pain/tenderness • Measure size • Finger breadth’s from costal margin • Liver span • Percussion • Auscultate • Liver hum: HCC • Hepatomegaly • Metastasis • HCC • Myeloproliferative • RHF • ALD • Haematological disease • Hepatitis • Fatty liver
Examining Ascites • From centre to flanks • Flanks will become dull, as fluid settled • Fluid thrill • Shifting dullness • Percuss to right flank of patient: dull • Ask pt to turn onto left side: wait • Re-percuss to right flank: resonant • Classifying Ascites: • Exudate (>30g protein/L) • Carcinomatous infiltration • Acute pancreatits • Infection • Transudate (<30g protein/L) • Portal hypertension • CCF • Nephrotic syndrome • Ovarian tumour
Examination of gallbladder • Below right costal marging, lateral border of rectus abdominis • Bulbous, focal, round mass, moves with inspiration • Murphy’s sign: cholecystitis • Painful palpation of right costal margin on inspiration • Courvoisier’s law: • Enlarged gallbladder and pt jaundiced, unlikely gallstones (gallbladder fibrosed) • Gallbladder enlargement • with jaundice: • Ca pancreas • Ca ampulla of Vater • without jaundice: • Ca gallbladder • Acute cholecystitis • Mucocele/ empyema
Examination of spleen • 2 hands: • Posterolateral left lower ribs • Palpate with right, start RIF • Features of spleen: • Moves with early in inspiration • Can’t get above • Notched edge • Dull to percuss • Enlarge towards umbilicus • Splenomegaly • Chronic liver disease: Portal hypertension • Infection: viral hep, cmv, infectious mononucleosis • Haematological disease
Other findings • Tender epigastrium: PUD • Succussion splash: gastric outlet obstruction • RIF pain, peritonism: appendicitis • Pancreatic pseudocyst • Aortic aneurysm: expansile pulsation • Virchow’s node: Gastric Ca
Finally... • Percussion • Auscultation • Bowel sounds • normal/sluggish/tinkling/borborygmi/absence • Friction rubs • Inflammation • Venous hums • Portal hypertension • Bruit • Chronic mesenteric ischaemia: mesenteric artery stenosis • To complete examination: • Hernias • PR • Urinalysis • Present positive findings and give differential diagnosis • To investigate this further I would...(as previous) • Routine blood/imaging/specific tests
Common OSCE stations • Spotters: • Stoma (later slide) • Abdominal scars • Laparotomy, appendicectomy, cholecystectomy • Remember laparoscopic possibilities • Jaundice: Liver cirrhosis, Hepatitis • Ascites • Ascitic drain • Clubbing: IBD, Liver cirrhosis
History stations • IBD • Peptic ulcer disease • Oesophagitis • Gallstones • Cholecystitis • Pancreatitis • Hepatitis • Colorectal cancer • Alarm Symptoms: • Iron deficiency anaemia • Weight loss • Progressive symptoms • Melaena/Haematemesis • Swallowing difficulty
Acute abdomen • Always SP for this station • Remember ABC!! • Focussed history • SOCRATES • Focussed abdominal examination • Present only positives! • Summarise • Differential Diagnosis • Investigations • Common scenarios: • Appendicitis • Cholecystitis • Pancreatitis
Stomas • An artificial opening in abdominal wall • Passage of waste: faeces/urine • Non-functioning/Mucous fistula • Temporary/Permanent • Single opening (A) or double barrelled (B) (emergency) • Why formed • IBD • Cancer • Trauma • Severe diverticular disease • Types: • Colostomy: flush with skin, solid contents • Ileostomy: spouted, porridge-like contents • Jejunostomy • Gastrostomy • Urostomy(with ileal conduit)
Stomas • Complications • Early: • Haemorrhage at site • Ischaemia • High output: electrolyte losses • Obstruction: adhesions • Retraction • Delayed: • Dermatitis • Prolapse • Parastomal hernia • Fistulae • Psychological: smell, relationship problems • Stoma Nurse Specialists!!!
Explanation stations • Explain chronic condition and/or management: • Iron deficiency anaemia: starting iron • IBD • Peptic ulcer disease: Triple therapy • Explain procedures • Colonoscopy • OGD • Biopsy • Breaking bad news • Not always cancer! • Chronic disease • Explain to relative
Interpretation • Liver function tests • Anaemia • Iron deficiency • Pernicious anaemia • Macrocytic • Hepatitis screens • Viral screen: A, B, C • HBsAg +ve 1-6 months (>6 months=carrier status) • HBeAg +ve 1-3 months:high infectivity • Anti-HBc +ve: past infection • Anti-HBs +ve alone: vaccination