Download
1 / 46
460 likes | 761 Views
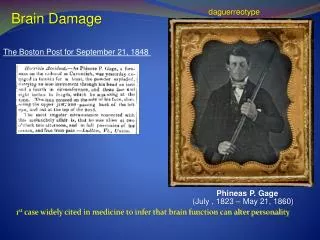
Brain function – the evidence from brain damage. Brain damage to a specific area and you cant talk? Maybe that area controlled speech?. Language Centres – Left Hemisphere. STUDIES OF APHASIA.

E N D
Brain function – the evidence from brain damage Brain damage to a specific area and you cant talk? Maybe that area controlled speech?
STUDIES OF APHASIA • “Aphasia” is a general term for clinical purposes to describe individuals with a language disorder apparent in speech (comprehension or production), writing or reading produced by injury to brain areas specialised for these functions. • Aphasic disorders do not include language disturbances due to severe intellectual impairment, loss of sensory input (vision or hearing), paralysis or muscle coordination impairment in mouth movement or hand. http://www.youtube.com/watch?v=ZJ4shANmIN8&feature=related
STUDIES OF APHASIA • Aphasias are often classified into 3 general categories: • Fluent aphasias – where there is fluent speech but difficulties in auditory verbal comprehension or in repetition of words, phrases, sentences spoken by others. • Nonfluent aphasias – Difficulties in articulating but auditory verbal comprehension is relatively good. • Pure aphasias – Specific impairments in reading, writing or recognition of words. Within each category there are numerous subtypes of aphasia (including Broca’s aphasia and Wernicke’s aphasia). Most common cause of aphasias is stroke.
Broca’s Area • Broca’s Area • Located in the frontal lobe of the LEFT hemisphere only • Production of articulate speech, clear and fluent • Moves the muscles that are required to speak • Involved in analysing the grammatical structure of sentences, helps us extract meaning from language
Broca’s Aphasia • Damage to Broca’s area – produces very deliberate speech consisting of a few words with very simple grammatical structure. Rarely results in total loss of speech. • Broca’s aphasia (non fluent aphasia, expressive aphasia or motor aphasia) = Trouble with speech production, speech consists of very short and simple sentences, mainly verbs and nouns but can still understand speech. • Small parts of speech (e.g. “to” and “the” are omitted as well as endings such as “ing” and “ed”.) e.g. Went house visit cousin. • Reading and writing not as effected (can be in some cases though) • Deaf people can sometimes have difficulty signing if Broca’s affected. Although this depends on whether they were deaf from birth…..
BROCA’S APHASIA • Some evidence that comprehension of speech can be impaired. Easily confused when usual order of words is changed, especially if meaning cannot be inferred from individual word meanings alone. E.g. The boy hugged the girl (is OK) but The girl was hugged by the boy (may be confusing) because meaning cannot be inferred from individual word meanings or by context alone. • Many studies also have failed to show a clear and consistent relationship between location of damage and the area originally described by Broca. However, damage is always found in left frontal lobe areas, indicating its role in speech production. http://www.youtube.com/watch?v=1aplTvEQ6ew&feature=related http://www.youtube.com/watch?v=f2IiMEbMnPM&feature=related
Test for Broca’s Aphasia ‘stool, is it boy, is it that landing down, girl is laughing, and cookie jar……….ok um…..window….curtains and out the garden and trees low grass and um lady washing the dishes and hot and cold water….plashing running, floor , and the two cups of a, two cups of ah, two cups of ah, coffee or um….empty um……..cupboard and cupboards …..um……washing…..flashing and um earth to roof’
Wernicke’s Area • Located in the temporal lobe of the left hemisphere only, next to the primary auditory cortex • Involved in the Interpretation of speech, referred to as the language comprehension center • Vital for locating appropriate words from memory to express meaning
Wernicke’s Aphasia • Damage to Wernike’s area • Wernicke’s aphasia (fluent aphasia, sensory aphasia or receptive aphasia) = Trouble with speech comprehension. Also cant produce meaningful sentences, can string words together but what they say is nonsensical. • Different to Broca’s aphasia as speech is often fluent and grammatically correct but what is said is nonsense. It often has the correct rhythm and general sound of normal speech but content is odd, conveys little information and sounds like a word salad. • Different to Broca’s aphasia, sufferers have little or no conscious awareness or understanding of their condition. They are unaware people don’t understand them. • Like Broca’s aphasia, most commonly caused by stroke. http://www.youtube.com/watch?v=aVhYN7NTIKU http://www.youtube.com/watch?v=dKTdMV6cOZw&feature=related
Test for Wernicke’s Aphasia ‘Mother is away here working her work to get her better, but when she’s looking the two boys looking in the other part. She’s working another time.’
Right hemisphere and language? • Research shows right hemisphere also has a role in language. • Patients with left hemisphere damage can sometimes still use emotive words and swear, or produce well learnt phrases or sing! • Emotion more a right hemisphere function • Also sometimes can sing what they cant speak making use of right hemispheric musical function. • Some frequently used concrete words (e.g. Car, television, food) are understood by right hemisphere even if patient is unaware they have been shown the word. • Right hemisphere appears to have the ability to comprehend the overall context or theme that is present in a sentence.
Neglect Syndrome Nothing on you left! Damage to the right!
Neglect syndrome • Also called spatial neglect, hemineglect, hemispatial neglect, contralateral neglect and unilateral neglect. Some of these refer to subtypes. • Damage to the right parietal lobe • Results in the patient completely ignoring the left side of their world, even the left side of their body. • Patients eat only the food on the right side of their plate, shave the right side of their face, wash the right side of their body etc. • A problem of attention, not blindness! • Most commonly observed in stroke or accident victims. • Can sometimes occur after similar damage to left parietal lobe, but much less frequently and in a milder form.
Neglect Syndrome • Usually occurs with visual sense but can occur in other senses such as hearing or touch, or with movement. Can be one sense or a combination. • Patients can confuse receiving the sense on the neglected side when it occurs on the right (e.g. A sound heard on left side when it actually came from the right). • Extra visual cues may attract patient’s attention towards neglected side so they may notice something they had not attended to before. • Most common feature though is apparent lack of awareness of the presence of anything on their left side.
Neglect Syndrome • The neglect can occur internally to “mind’s eye” as well as external world. • Bisiach and Luzzatti (1978) – 2 neglect patients close eyes and imagine standing at a famous landmark in Milan well known to patients prior to their stroke. When describing the landmark they noted details on right hand side of imagined gaze and not left items. A control group identified both sides with similar number of errors. This suggests spatial neglect can affect recall of images from memory but does not involve memory impairment.
Neglect Syndrome • Extent of neglect depends on severity and location of brain damage. Can range from indifference to objects on one side to denial of existence of that side of body. • Psychologists are unclear why it occurs following parietal lobe damage but it indicates importance of right parietal lobe in attention and conscious awareness of objects internally and externally. • However, many other brain areas are also involved in attention and consciousness – frontal lobe, RAS and thalamus. • Some patients make a gradual recovery from the disorder. • http://www.youtube.com/watch?v=ADchGO-0kGo
Split Brain Surgery Sounds cool until your brain is cut in half
Split Brain Surgery • Severing the Corpus Callosum • Used to treat severe epilepsy • Disables communication between the left and right hemispheres • Leads to visual deficits • http://www.youtube.com/watch?v=MZnyQewsB_Y
Split Brain Studies • Gazzaniga’s split brain test and research http://www.youtube.com/watch?v=0lmfxQ-HK7Y • Split brain behavioural experiments (Gazzaniga) http://www.youtube.com/watch?v=ZMLzP1VCANo Nobel prize website animation http://nobelprize.org/educational/medicine/split-brain/about.html
Split Brain Test • Object presented to left visual field (processed in right hemisphere) • Cannot name object • Can pick correct object up • Object presented to right visual field (processed in left hemisphere) • Can name object • Conclusion – language processing occurs on LEFT
Information from left visual field is processed in the right hemisphere • Information from the right visual field is processed in the left hemisphere
Things to do • Learning activities 4.14, 4.15, 4.17 • Chapter Summary
Perceptual Anomalies Are you sure what you see is real?
PERCEPTION • Perception occurs when sensory information reaching the brain is meaningfully interpreted. Based on what we see, hear, smell, taste, touch etc. our brain actively processes and constructs reliable representations of reality; allowing us to adapt to our environment and make sense of a constantly changing world. • Our perceptions are an important aspect of our conscious experience. • Perception often closely matches the physical world around us, but NOT ALWAYS is perception error free! Sometimes we experience perceptual anomalies.
PERCEPTUAL ANOMALIES • A perception anomaly refers to an irregularity in perception. • It involves an inconsistency or “mismatch” between perceptual experience and physical reality. e.g. Driving on road see a “puddle” glistening on road some way ahead, but as continue driving you see road stays dry and the “puddle” is still in the distance. This visual illusion is caused by a layer of hot air beneath cooler air that casts a reflection from the sky onto the road.
PERCEPTUAL ANOMALIES • Perceptual anomalies can occur with senses other than vision. e.g. • Pain can persist longer than causing injury has healed. Also amputees can perceive chronic pain from an amputated limb. • Can hear things that may not exist in reality. • Can perceive taste in something with no chemical basis for what is tasted. • Can perceive movement that isn’t real (moon moving across sky when clouds pass in front of it on a windy, cloudy night. Adjacent vehicle moves forward, you momentarily feel like your vehicle is moving backwards.
Motion after effect • 1834 philosopher Robert Addams staring at Falls of Foyers in Scotland experienced what he later called the “waterfall illusion” - now referred to as “motion after-effect” • Motion after-effect is the perceptual illusion of the movement of a stationary object following exposure to visual motion • The stationary stimulus appears to move in the opposite direction to the original stimulus. • Movie scrolling credits – don’t follow names, focus on fixed point at centre of screen then at the end of the credits you will experience illusory motion in opposite direction to the scrolling. • Cause is not fully understood • Seems clear that eye movement and neurons in the visual cortex specialised to detect and respond to motion are both involved.
Motion after-effect • Neurons in visual system sensitive to the direction of movement are located in the retina of the eye and visual cortex at the back of the brain in humans. • Prolonged exposure to a particular direction of motion may make neurons in the visual cortex involved in detecting motion in a particular direction to become fatigued and fire less, reducing their responsiveness to movement in that direction. • Neurons responsible for motion in the opposite direction are not fatigued and fire normally, thereby producing the “motion after-effect”. • The result is that the activity of one set of neurons is not balanced out by the other and ‘false’ motion is perceived briefly until the fatigued neurons recover .
Motion after-effect • Despite this potential confusion, we consciously experience a seamless, organised, stable and coherent world. Perceptual processes have a critical role to play in this outcome. • Illusions such as “motion after-effect” indicate that perception may be reliable but does not always reflect reality.
Akinetopsia (motion blindness) • A rare disorder resulting from brain damage where an individual is unable to perceive motion in many aspects of their visual world. • E.g. German adult female referred to as “LM” who saw the world almost entirely as a series of “snapshots” rather than moving images, especially if movements were quite fast. • Crossing the road, pouring tea, following conversations, moving in a crowded room. • She could locate and perceive stationary objects so was able to control her eye movements, but tracking with eye movements was abnormal. • There is no effective treatment for akinetopsia. http://www.youtube.com/watch?v=B47Js1MtT4w&feature=related
Change Blindness • The failure to see large changes that should be noticed easily is referred to as change blindness. • Research indicates we can experience a remarkable lack of awareness of events that take place in our visual environment. • The change must take place during a brief visual disruption (can include eye movement involving retinal disruption) • Change blindness occurs both when change is expected and unexpected, although when expected we may eventually detect the change but it can take a long time to do so. E.g. Flicke3r technique of two pictures and told to find the one change with a blank screen in between briefly (80 milliseconds) See Fig. 4.49 on p. 230 • Change blindness effect is even stronger when changes are unexpected.
Change Blindness • Looking at an object is alone not enough to guarantee perception – attention clearly plays a role • If attention and mental effort are not made to create a cognitive representation of the scene then as soon as visual memory fades (0.3 of a second) then we have nothing to compare the new image to and thus do not notice any difference • Highlights the importance of ATTENTION and SHORT TERM MEMORY in perception • Just seeing an image is not enough
Inattentional Blindness • Change blindness is different from “inattentional blindness”. • Inattentional blindness (e.g. Gorilla presence across ball game) • Inattentional blindness is a failure to notice something in a scene when the same scene continually remains in sight. There is no visual disruption or any reliance on memory.
Inattentional Blindness • Not the same as change blindness • No disruption • Ability to notice change is limited particularly if attention directed at a specific object or event (eg. Ball passers research) • Sometimes we know something is changing but cant tell what. Research by Rensink (1998) using flicker technique and participants indicated awareness of something changing but not clear on what. They did not visually experience the change but reported a “feeling” that something had changed. Rensink (2000) believes this provides some evidence for a phenomenon known as “mindsight” – the feeling of “seeing” with no accompanying visual experience. • The visual information is present but we cannot notice or latch on to it
Change blindness • Studies on change blindness make it clear that our focussed attention is needed to detect any change in a scene. Although focussed attention does not guarantee we will detect the change, even when it is large or expected.
Blind sight? • Under research conditions some people report being able to ‘feel’ that something is changing even though they report being unable to ‘see’ anything change. • V.S Ramachandran and his ‘blind’ patient • Reminds us that whatever is going on simply having a functioning visual system is not enough. Attention and consciousness play a major role.
Synaesthesia • Synaesthesia is a perceptual experience in which stimulation of one sense produces additional unusual experiences in another sense. • The additional sense experience “adds” to overall perceptual experience without replacing the initial sense. • It is a real experience that has some characteristics: • Involuntary • Occurs automatically in response to relevant sensory stimulation • Extremely difficult to suppress • Vivid, highly memorable experience • Consistent experience across time
Synaesthesia • Stimulation of one sense produced additional and unusual experiences in another sense • For example the number 3 will always appear as blue regardless of its actual colour – this is known as grapheme-colour synaesthesia • Tends to be one way rather than bidirectional (sound produces a taste, but taste doesn’t produce the sound) • Effects roughly 1 in 2000 • Unclear as to why it occurs – possibly synesthetes are unusually sensitive to external stimuli • excess of neural connections not pruned after early childhood thus synesthets retain these neural connections • neural wiring that is unusual – i.e. neighbouring sensory areas being cross wired
Synaesthesia • Synesthetes thought to have differences in architecture of brain, but not structural and/or functional brain differences. i.e. Brains are wired differently so that neighbouring sensory areas in brain cross-activate one another, thus triggering additional sensations. • Neuroimaging technology is helping somewhat in supporting this theory. • Researchers study synaesthesia not only because it is a perceptual anomaly but because it may shed new insight into how the brain is organised and cognitive processes in perception and consciousness.
Synaesthesia • May be a genetic basis as to its experience, as it tends to run in families. • No strong evidence for gender differences in its experience. • Some forms of synaesthesia are more common than others. • Common: seeing colours produced by sounds, or seeing letters in specific colours. • Uncommon: smell produced by touching a particular shape, or a taste produced by hearing words.
Things to do • Learning activities 4.14, 4.15, 4.17, 4.18, 4.19, 4.21 • Chapter summary!