Download
1 / 55
700 likes | 1.37k Views
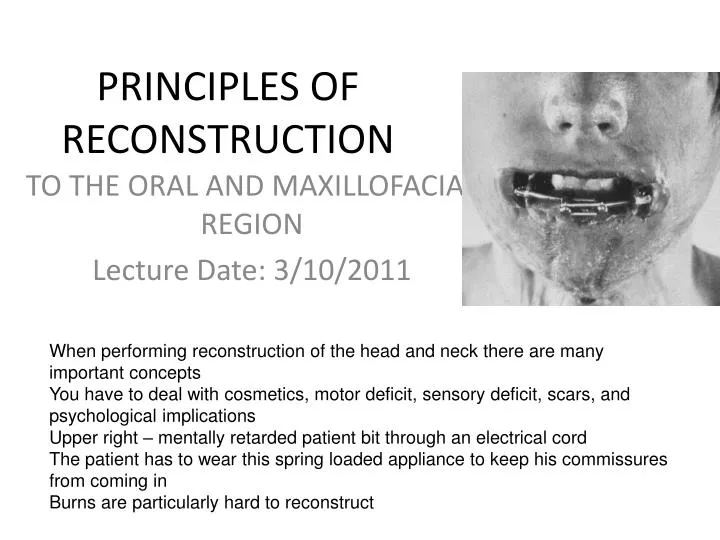
PRINCIPLES OF RECONSTRUCTION. TO THE ORAL AND MAXILLOFACIAL REGION Lecture Date: 3/10/2011. When performing reconstruction of the head and neck there are many important concepts You have to deal with cosmetics, motor deficit, sensory deficit, scars, and psychological implications

E N D
PRINCIPLES OF RECONSTRUCTION TO THE ORAL AND MAXILLOFACIAL REGION Lecture Date: 3/10/2011 When performing reconstruction of the head and neck there are many important concepts You have to deal with cosmetics, motor deficit, sensory deficit, scars, and psychological implications Upper right – mentally retarded patient bit through an electrical cord The patient has to wear this spring loaded appliance to keep his commissures from coming in Burns are particularly hard to reconstruct
RECONSTRUCTIVE CHALLENGE • Patient was shot and then sent to jail and was never reconstructed • Clinical characteristics: • Shot through the lower jaw, lost lower facial form and lip competence • Commissure is off • Motor deficit, ptosis of the left lower face • This will take many surgeries to fix and he’ll still look funny at the end • The best reconstructive options will always be an immediate reconstructive option • When you don’t do an immediate reconstruction you have a lot of scar formation to deal with as well as loss of function
DEFECTS OF THE FACIAL BONES • TYPES (5) 1. Congenital 2. Pathologic 3. Trauma related 4. Infectious 5. Acquired • As it goes to what is the easiest to reconstruct, we find that the congential defect is probably easier to construct because you don’t have to go through the tissue trauma type concepts to fix the patient • The most common defect seen is the acquired, usually secondary to pathology or trauma
Each defect poses its own unique challenges • This patient didn’t have their seatbelt on and went through the window when she hit a tree • Soft tissue trauma, bone abnormality, most likely salivary gland, parotid duct and facial nerve injury • Trauma is down to skull in forehead area – have to worry about frontal sinus • Also has vascualarity and nervous consequences
MOST MAXILLOFACIAL DEFECTS • We must provide osseous reconstruction to get appropriate soft tissue drape • With that said, the most important concept as it relates to reconstruction is vascularity of the soft tissue bed. • If it doesn’t have good blood flow you won’t get adequate bone healing Will have both an osseous and soft tissue component
OSSEOUS RECONSTRUCTION • What part of the face has been affected? • The mandible becomes an important bone to reconstruct because it has many things it does • Functions of the mandible: a) Facial contour • Gives vertical dimension of the face in the condyle-ramus area • From the ramus to the chin it gives projection of the face b) Facial support • Important for facial support because it is the key to build the occlusion c) Muscles of mastication • The muscle of mastication are attached to the mandible, so the patients ability to masticate is directly related to how much mandible is present d) Tongue/Floor of mouth • All of the tongue muscles attach to the inferior mandible. If they aren’t attached deglutition or swallowing is affected e) Muscles of facial expression • Muscles of facial expression are attached by facial attachments to the mandible, so the face doesn’t move it the mandible isn’t complete
INTRODUCTION TO THE CANCER RELATED DEFECT • NEEDS: Bone Soft Tissue Augmentation of existing ridges Removal of scar and mucosal encombrances • Scar – keratinized tissue might need to be brought in Restoration of facial form People who undergo head and neck cancer removed will have the prototypical defects we see
BONE GRAFTS • Healing of bone is unique: new bone arises from tissue regeneration with cellular proliferation (osteoblasts) and collagen synthesis • Obviously we need to graft viable live cells when doing bone grafting • Remember the osteoblast forms new bone and the osteocyte is what provides bone stability to intercommunicate with other bone cells • Ultimately you get collagen synthesis and calcification of the boney structures • Bone grafts come from several areas • Marrow bone grafts bring in osteocompetent cells • You can also bring whole pieces of bone, muscle, and vessels • The best way to do it now is by free tissue transfer where you bring bone, soft tissue, and vascularity and plug it into the head and neck
BONE HEALING CONCEPT Vascularization 2 Phases of Healing Axhausen 1956 • This was before we could use the fibula to make a new jaw bone
PHASES • Phase 1: starts from transplanted cells in the graft that proliferate and form new osteoid. Determines the quantity of surviving bone • Phase 1 is what determines the quantity of surviving bone • Phase 1 bone growth is affected by what you put your graft material in before you put it in the patient’s body • Do you take your bone marrow out and put it in sterile water? D5W (dextrose 5% water)? Normal saline? • Saline – because it is isotonic (it’s the best material to put your bone graft in before putting it in the patient) • If you put it in water or D5W you will see the bone cells burst and you won’t be able to transplant viable cells into the graft site • Phase 2: consists of the classical resorptive remodeling process- no new quantitive bone is formed • What is the difference between bone marrow and cortical bone? • Bone marrow is where the live good osteoblastic cells are located • Cortical bone has mature cells or osteocytes • You must have some cortical bone in your graft because it provides BMP (bone morphogenetic protein)
Healing overview Superficial cellular elements survive by nutrient diffusion • When you first put your bone graft in you get nutrient diffusion from the surrounding area • Thus the basis for graft survival is associated with how healthy the soft tissue bed is, because that is where the nutrient diffusion is from Hematoma formation • You then get hematoma formation • This is associated with what type of hemopoetic cell? • Platelets • You get a blood clot and then platelet derived growth factors Granulation tissue ingrowth • Granulation tissue ingrowth means angiogenesis – the starting of budding of the blood vessels Prominent vascular and mesenchymal cellular components ie OSTEOINDUCTION • Then you see the small arterioles become small arteries
Healing con’t • Osteoclastic activity allows further vascular invasion. • Vascular invasion = angiogenesis • Osteoinductionoccurs:mesenchymal tissue differentiates into tissue capable of osteogenesis-regulated by BMP • Where do we get BMP from when we incorporate a bone graft? • The cortical bone • Osteogenesis with repair and incorporation of graft = final phase • Once the graft is put in your soft tissue bed is the most important thing related to bone survivability • No good soft tissue bed – your graft won’t survive • Bisphosphonates work by affecting one of the cells that occur in bone • The three cells are osteoblasts, osteoclasts, and osteocytes • Bisphoshonates turn off the osteoclast • They also may affect osteoblastic activity on occasion • It is the osteoclast that allows further vascular invasion so the graft becomes vascularized • We now have BMP wafer that we can use for bone grafting • When you use BMP that is produce commercially it causes a reaction within the tissue • It makes a bunch of bone but as a side effect it causes significant swelling • Osteogenesis – forming bone from mesenchymal differentiation or from bone placement in there • Osteoconduction – putting bone structures in place but it is only acting as a scaffold • Best when you can do osteoinduction and osteoconduction at the same time – gives a better and denser bone graft
ACTIVATION OF BONE REPAIR • Occurs by local and systemic factors • Parathyroid hormone: most potent agent to stimulate remodeling activity. Stimulates pluripotential cells (elaborates osteoclasts). Ca++, GH,thyroxinstim. activity. Calcitonin,estrogen, adrenocortical steroids inhibit activity • PTH – Ultimately the osteoclast development is stimulated by PTH. • Other types of hormones we see are calcium • We tell patients that undergo head and neck reconstruction to take calcium, we prescribe it at at least 4000 units. In osteopenia and osteoporosis patients we tell them to take vitamin D3 at 1000 mg a day in addition to the calcium. • Inhibitors: Calcitonin, estrogen, adrenocortical steroids • If you do a big reconstruction and you suspect a lot of swelling or your expect to be close to the nerve and you don’t want to cause nerve injury you will give the patient decadron (steroid-like). This affects overall bone graft maturation.
BONE FORMATION Stimulated by growth factors
TRANSFORMING GROWTH FACTOR-BETA SUPERFAMILY • Osteogenin BMP-3 • BMP-2A • BMP-2B • BMP-5 • BMP-6 • Osteogenic protein BMP-7 • TGF-B1-5 • Vg-1Activin Beta A & B • Inhibin alpha • Decapentaplegic complex • Mullerian inhibiting substance
Notes on the TGF-Beta Superfamily • Underactive research now • You will see that we are utilizing BMP pledgetts for bone grafts, they are a great source of bone graft material and activity • Pledgett = a little wafer, when purchased they ask what size you want and you give that to them in millimeters. It is thin and is a chalky like substance when you put it in. • One problem he has is taking body parts to make body parts, like taking a fibula to make a mandible, etc • If the patient gets infected and loses the graft, they lose that body part • We are starting to see bioengineering as it refers to the head and neck, especially related to BMP • The biggest problem we have with BMP is that: • It is expensive. To get a pledgett you will spend $150-$1,000 • When you put it in it grows gorgeous bone. But you also see a horrible salytic process, so the patients face swells. The swelling starts about a week or so after you put it in and stays 4-6 weeks. This pisses the patient off. • BMP is classically located in cortical bone not cancellous bone.
TGF-B SUPERFAMILY • Overall Function: osteogenesis, chondrogenesis, wound healing, fx healing, cellular differentiation ie multifunctional growth factor • Sometimes we take patient’s blood, spin it, and make platelet-rich plasma • PRP is an adjunct to your graft • Bob Marx came up with HBO, PRP, and an test to see if you are susceptible to bisphosphonate-related osteonecrosis • HBO is a very expensive treatment. We now are seeing studies come out that says that HBO doesn’t work. He’s wondering why he got so many patients to heal with osteoradionecrosis. HBO is falling out of favor. • Patient: Metastatic prostate cancer, previously had full parotidectomy and radiation. He now needs 10 teeth out, what do you do? Do you send this patient to HBO? • HBO causes blood vessels to grow in the bone. With this patient you would be stimulating the further growth of cancer in the bones of this patient. So no you would not send them there • PRP is injected over bone graft. The idea is that there is relative increase in the amount of platelets, and therefore an increase in platelet-derived growth factors which would give you a better graft. • That doesn’t really work. You get a harder bone graft at first but later on it is not any stronger than if you had done this without the PRP. • Tara A… from UMKC proved that it didn’t work • Bisphosphonate-related osteonecrosis test • Marx thinks this test can give you an overall image of osteoclastic activity in the body. • Most scientists disagree. He was pushing this because he is part owner of the company that does the testing
TYPES OF GRAFTS • Vascularized ie osteomyocutaneous • Nonvascularized cortical cancellous other:bone slurry,particulate bone bone paste(paté) corticocancellous
Notes on Types of Grafts • You will see the nonvascularized most • The state of reconstruction is showing us that for any major defect an osteomyocutaneous graft will give you better vascularity and will be resistant to infection. In addition it works very will in radiated tissue because you are increasing vascularity in the area, increasing vascular bed blood flow. • Cortical grafts are hard bone so structurally they give you strength to your reconstruction, but they have to be fully decorticated by the body before you can have new bone. With cortical bone you typically do not graft live cells. • Live cells are contained in the cancellous portion of your bone graft. Cancellous grafts have osteocompetent cells and they provide an ease of penetration of the BV. So vascularity is much quicker and more complete in this graft. • The best nonvascularized graft one can use in the body is a combination of cortical and cancellous.
CLASSIFICATION BY STRUCTURE • Cortical • Cancellous • Corticocancellous • Cortical vscancellous re: ease of vascular penetration • This is the difference between the two • Cortical bone is very important because it contributes to the phase 2 portion of bone healing and that is directly related to the amount of BMP in the cortical bone
CLASSIFICATION BY ORIGIN • Autogenous/Autograft • The standard bone graft we like to use that is considered the best is the autogenous bone graft, these are also referred to as autograft • He will ask this on the final because it is a definition question, tends to be on boards • Allograft/Isograft/Homograft:one individual to another of the same species. Lyophilized—reconstitute • Allografts are the same species, so a cadaver bone would be one • All allografts have to be hydrated. This hydration is referred to as reconstitution and is typically performed with saline. You will see that they may ask you in the package insert to put in a capsule of tetracycline with the allograft. He isn’t sure if it makes a difference but he would do it. You place a 500 mg capsule. • Xenograft:tissue transplant from 1 species to another. Bio-Oss/Osteogen • Xenografts are from one species to another, typically bovine. Classic example is Bio-Oss • Alloplasts:Inert synthetic materials • Alloplasts or synthetic materials are usually of the hydroxyapatite family. So ceramics are alloplasts used in reconstruction, typically in implants.
Notes on Donor Site Volumes • YOU WILL SEE THIS AGAIN • If you are using autogenous bone what are the largest bone stocks you can access? • The amount of material you need to reconstruct determines where you pull the bone from • Anterior iliac crest – that is right where your underwear is, its where you lay down when on your side, and there are muscles that attach there that help swing your legs • This is a gorgeous site to get to, very easy. But it has some problems if you do it wrong. • These are very painful afterwards • Looking at this you can go medial into the pelvis, one problem with this is you are close to the sacroiliac joint causing an unstable pelvis • This will give you 30-50 cc of bone • The largest reservoir of bone can be harvested from the posterior iliac approach • The calvarium gives you minimal amount of bone, the best bone there would be on the outer cortical plate • If you need bone marrow, where is the bone marrow in the calvarial bone graft? • It is located in the diploid space – the space between the outer cortical plate and the inner cortical plate. • He thinks the rib is a horrible donor site for almost all applications in the head and neck. The only application that he thinks is reasonable is the costrocondral graft to reconstruct the TMJ. • A reasonable donor site to reconstruction the TMJ would be a costrocondral graft. Usually taken from the contralateral side. So if you are doing a right condyle you will take a left rib. You usually take ribs either 4 or 6 • Complications associated with bone grafts: • Anterior iliac crest – numbness in the pelvis • An ilieus – bowels stop their parastaltic movement, this usually goes away in about a day • A way you would determine if a patient has this is if they don’t have bowel sounds • Disturbance in gait (hip graft walk) – may need PT to help them go up steps • Posterior iliac crest – usually minimal • Pain and a disturbance in the gait • Calvarium – scar in the scalp needed to access bone • Usually performed in the parietal bone • Ribs – pneumothorax • This means you have violated the pleural cavity. Therefore you can drop a lung
ALLOGRAFTS • Are osteoconductive (no viable cells) • Packaged in a lyophilized state and must be reconstituted • exam: freeze dried, demineralized bone • Offers only a hard tissue matrix for the inductive phase of healing (no viable cells for osteogenesis) • Allografts are relatively resistant to becoming infected if you have a great soft tissue bed • There is a discussion – if you use an allograft and you place it through the mouth rather than through a neck there is a high potential for it being contaminated • Not uncommonly he will give the patient antibiotics afterwards for prevention of the infection process. He gives at least 7 days but usually 10 days
Cadaver Mandible • Comes in small, medium, and large • When you get it comes in a package. You must hallow it out and then perforate it with the holes to allow vascular ingrowth • He hasn’t figured out how to hallow out the neck without it breaking when you put it in the body
He then takes his hip bone and fills the cadaver crib and places it • This works but now well because all of the cadaver bone must be resorbed before new bone is made • He finds that it never heals and the anterior junction where it comes in contact with the native bone • He also has found that it is hard to keep the donor bone up in the glenoid fossa. It will be good when placed but after 24 hours it begins to sag. He has tried using a suture to keep it in the fossa but it tends to pull it the wrong direction.
SOFT TISSUE BED • Is the key to reconstruction of head and neck patients • Fibroblastic cellularity and vascular density determine the quality of the recipient bed • Concept of ORN and HBO - already addressed • When you receive postop radiation what does it do? • It affects cells in the middle so that it ultimately affects cells and stops mitosis. • Radiation induces an inflammatory process associated with the blood vessels called indarteritis. This causes a relative decreased blood flow, so that you then have hypoxia of the tissue. In conjunction with the hypoxia you have decrease cellular turnover. • We call it the 3 H’s – hypovascularity, hypoxia, and hypocellularity • So once the radiation is given it is indiscriminant. So now to reverse that process they have come up with HBO. • The classical description of HBO is that you place a patient in a chamber and you pressurize the chamber. In fact the pressure in the chamber is 2.4 atm. You need to submit a patient to depth daily for 6 weeks. 6 weeks is 30 dives. You are at depth for 90 minutes a day. • Somewhere around dive 13-15 the amount of oxygen in the tissues (referred to as the PaO2) is approximately 80% of normal. You will typically take a patient through 20 dives initially, then he has surgery, then he goes back for 10 more dives postoperatively. • Medicare will not pay for this unless you have ORN, so you can’t use this in a preventive manner to stop it • A patient going through this will tell them that they can see better – it stimulates retinal growth, this is only temporary • They may tell you they can’t hear as well because it increases pressure in the inner ear • This costs $1000 per dive, so $30,000 total • There was a study out 3-4 years ago by MD Anderson in Texas where someone did over 2000 extractions on irradiated patients and studied the incidence of ORN. It was pretty low
State of the Art: Bone grafts? • Primary cancer resection with post-op RT • Wait 1 year • Not reasonable because the patient is not whole, the concept of wholeness to the patient is very important psychologically and physiologically • You also end up with a lot of scarring which affects your ability to reconstruct • Hyperbaric oxygen protocol with allogenic crib and iliac crest PCBM mandibular reconstruction • Wait 4-6 months • Same process, patient is not whole, not eating and feeling well, poor soft tissue bed • Vestibuloplasty and placement of osseointegrated implants • Wait 4-6 months • Also a problem • Prosthetic reconstruction Marx, RE. JOMS, 1995
Who Needs Bone? • Pre- free flap era • 46% success rate with non-vascularized grafts in primary mandible reconstruction • Success improved to 90% with delayed repair when graft placed extra-orally • Multiple surgeries required • Limited number of patients achieved functional reconstruction • These grafts are put in right after cancer was taken out • Horrible success rate • If they left the intraoral communication heal and then come back and graft the success rate is 90%, you also wouldn’t want to do this it has a 10% failure rate • Typically you see that the patient will come in with ORN and a draining fistula in the neck Lawson, W, et al. Laryngoscope 1982
TIMING OF RECONSTRUCTION • Two choices a)Delayed: wait a period of time post-ablation and then return patient to OR for reconstruction(usu. 6 months) Radiation, scarring, contracture,muscle atrophy, increased hospitalization,poorcosmesis and fibrosis can contribute to a suboptimal result • 6-12 months or longer • Looks bad • Fibrosis means you ultimately don’t get good bony union or heal • This is a poor concept
DELAYED RECONSTRUCTION • Due to masticatory muscle pull, typical distractive forces produce an upward and medial rotation of the bone segments • If you have a resection and you have a continuity defect you will have masticatory muscle pull • If that happens you have to re-align it and the patient will have TMJ problems after • The primary advantage of delayed reconstruction is to avoid wound contamination by saliva
TIMING OF RECONSTRUCTION • b) immediate: primary reconstruction is best accomplished by free tissue transfer with less scarring, fibrosis, fewer hospitalizations, and decreased complication. Will see clear benefits with respect to cosmesis, oral competence, deglutition/mastication, speech, sense of wholeness and dental rehabilitation • Probably your best option • If you are going in for a malignant resection you will see the gold standard now is free tissue transfer • A bladed surgery (the surgery to cut out the cancer) usually takes 4-6 hours, free tissue transfer takes 4-5 hours. So you usually have two teams, the first team removes the cancer and the 2nd team is on the extremity bringing the fibula, its muscles, skin, and blood vessels up to reconnect it to the system. • Oral competence – lips comes together • Helps with dental rehabilitation • We have tried to bring the fibula up, put in implants, and then put it in the mandible • The problem is the implant directionality is off • The best thing is to put the bone graft in, let it heal, then do implants
IMMEDIATE RECONSTRUCTION • Immediate single-stage reconstruction is always preferable to delayed reconstruction • Prevents development of muscle contracture
ONCOLOGIC RECONSTRUCTION • 20,000 NEW CASES OF ORAL CAVITY CARCINOMA OCCURS ANNUALLY IN US • Primary mode of treatment is surgical, and 50% of oral cavity cancers are in the advanced stages • Even today the 5 year survival rate associated with head and neck cancer is 50%
MICROVASCULAR FREE TISSUE TRANSFER • Can tailor the donor flap to the specific needs of the ablative defect • Concept – tailor flap to defect • They used to do pectoralis grafts, you would swing the graft up and onto the face. It would cause something looking similar to torticollis. • Not restricted by arc of rotation • With bone-containing flaps, resorption is minimized • With nonvascular cortical grafts you expect 20% resorption • Possibility of neural anastomosis • With microvascular transfer they can actually do things like make the tongue sensate (not fully but it will have some sensation) • Only true contraindications is hypercoagulable states • Anatomy problems are also a contraindication • Can you take a fibula graft in someone who has peripheral vascular disease? • No they may lose their feet (this is common with diabetics)
ARTERIAL AND VENOUS ANASTOMOSIS • Arterial connections into external carotid artery system, most commonly the facial artery, and also the superior thyroid artery • On occasion you may see someone use the lingual artery • These arteries give you nice length • Recipient veins include the internal and external jugular veins, facial veins, or cephalic vein from arm • You need both an artery and a vein when doing free flap surgery • The biggest problem with free tissue transfer is venous outflow • Right where you sew the veins together you see a little bit of collapse • You have to do flap checks – someone will have to use a stethoscope once an hour to hear the blood flow through the artery in the flap • If it becomes engorged the patient will have to go back to surgery to declot the vein
IJ (pink, flat) and EC (yellow) are next to each other • You can hear the EC bleed • It is covered by the SCM and the spinal accessory nerve runs across it
COSMETIC UNITS OF FACE • Noses – anything in the central face is particularly difficult to hide. For face reconstruction noses are particularly hard to make. • Eye – anytime dealing with the eye itself you will use an ocular prosthesis to restore the area • Lateral forehead, temporal region, glabella are all good for soft tissue and hard tissue reconstruction • The lateral mandible is usually best restored with the fibula • We are now going against basic hip grafts to restore the face
MANDIBULAR RECONSTRUCTION • Resection of mandible produces deformity and disability: facial contour/support; mm of mastication/facial expression,tongue/FOM support • Also, airway concerns: site of insertion of suprahyoid musculature which elevates the larynx and prevents aspiration; mand. supports tongue and thus the oral airway • The mandible is very important because it is the insertion point for the throat musculature – geniohyoid, thryohyoid, etc • It is also a site of insertion of the muscles of facial expression • The tongue in particular, you will have problems with swallowing • Airway concerns – if you resect the mandible, on occasion the patient has problems with respiration • The suprahyoid muscles elevate the larynx and when this is done it closes off the esophagus. Patients who have mandibular resection are at a particular risk for aspiration. These patients may aspirate in such large amounts that they end up with pneumonia. • Expect pneumonia if in the ICU more than 5 days
MANDIBULAR RESECTION • Mandible can be resected: subtotal or marginal, continuity defect, anterior/lateral/angle/condyle-ramus unit • Submarginal resection means the inferior border is intact • Continuity defect – you have taken the whole border of the jaw out, superior and inferior border are gone • If you take out the anterior mandible and you do not reconstruct it, it is called an Andy Gump deformity • Lateral and angle you can use the fibular to reconstruct that. That is true of the anterior mandible also. • Remember on the condyle-ramus unit we typically use a costrocondral graft (rib-cartilage unit) • Primary free tissue transfer usually by fibula osteoseptocutaneous flap(peroneal vessels) or the iliac flap based on the deep circumflex iliac vessels • The fibula free flap is the most common graft used to reconstruct. The other flap you can use is the hip bone flap or iliac flap. • He will not ask which vessels are associated with it. • RIGID FIXATION MANDATED • Anytime you do reconstruction of the head and neck you have to utilize rigid fixation. When we put plates on patients skeleton they come in different sizes. Rigid fixation implies that the plate is 2 mm thick or thicker. To do rigid fixation you must have three screws on either side of the defect.
MANDIBULAR SYMPHYSIS AND ARCH DEFORMITY-ANDY GUMP • If you have a contamination you lose a body part - problem
Anterior Defect • No reconstruction • “Andy Gump” deformity • Loss of lip support • Loss of oral competence • Loss of function and cosmesis– problems with articulation, phonation, and with eating • These patients have a problem with obstructive sleep apnea when laying back in bed
ANDY GUMP DEFORMITY • Resection of the mandibular symphysis/ anterior mandibular arch • Oral competence suffers from the patient’s inability to manage oral secretions, speak,eat, or swallow • Most important deformity to reconstruct primarily
OTHER MANDIBULAR DEFORMITIES • Posterior-lateral mandible, angle, and the ascending ramus defects can be effectively treated with free tissue transfer or with conventional techniques • A reasonable option for the condyle-ramus is a costrocondral graft
EXTIRPATIVE DEFECTS • Mandibulectomy defects • Replace with an osteomyocutaneous flap (bone, muscle, and skin) • Maxillectomy defects • Doesn’t set itself up well for free tissue transfer. Maxillary defects are best reconstructed with an obturator appliance. Very similar to a denture that replaces the anterior and posterior maxillary walls and the palate. • Glossectomy defects • Particularly hard to treat. The biggest reason is because the tongue is responsible for articulation, the swallowing mechanism, and because it is highly sensate. When you cut it out you lose all of that. So you don’t want to put a piece of muscle in there that doesn’t move, has no sensation, and so they can’t speak. This is typically treated with radial forearm flaps. • These can be quite difficult to deal with. • Defects resulting from excision of oral lining tissues i.e. floor of mouth,pharyngeal wall and cheek • If you are taking out anything that is the lining tissue you need to put lining tissue in to reconstruct.
GOALS OF SURGERY • Goals of Mandibular Reconstruction • Restoration of continuity • Restoration of alveolar bone height • Restoration of osseous bulk • Restore the bone in bulk and the alveolus • That is the problem with non-dental people doing head and neck reconstructions. They put they bone where you can’t use it. • Maintenance of osseous content over time • Restoration of acceptable facial form
Mandibular reconstruction with allogeneic crib/PCBM • Andy Gump procedure • He took a cadaver mandible, hollowed it out and cut the condyles off, packed it, and placed it in this woman. • Several hours after procedure the patient had a heart attack causing a loss of blood supply to the graft so he lost the whole flap
Mandibular reconstruction-Free tissue transfer • He took a piece of fibula out and took the vessels with it to reconstruct the mandible. • When doing reconstruction and ablative surgery you typically have two teams. One to take the tumor out and one to bring the flap up.
MAXILLARY RECONSTRUCTION • Try to achieve three (3) goals 1. Restoration of facial form-support for the orbital contents, cheek and lip • You must support the orbit • Remember the roof of the maxilla is the floor of the orbit. • You obviously have cheek and lip concepts associated with this. 2. Separate sinus/nasal cavity from oral cavity • You also must separate the sinus and nose from the mouth, no one wants snot constantly dripping into their mouth. He puts a barrier between the sinus and mouth to prevent that. 3. Dental rehabilitation • Ultimately consider a dental reconstruction
MAXILLECTOMY DEFECT-OBTURATION • Huge myxoma taken out of teenager • Utilized an obturator on one side with a metallic palate on the other side that is toothborne. • He is able to phonate and eat like normal with this, without it he wouldn’t be able to