Download
1 / 12
170 likes | 469 Views
Insulin Resistance. Progression to Diabetes Part 3. Optimal insulin sensitivity and protection against diabetes and CVD.

E N D
Insulin Resistance Progression to Diabetes Part 3
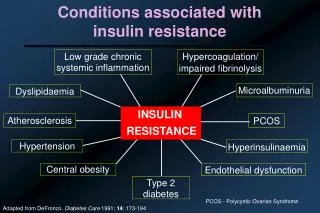
Optimal insulin sensitivity and protection against diabetes and CVD. • Note: Normal adiponectin can co-exist with glucose intolerance in very lean individuals. False–normal adiponectin can occur with renal railure or insulin receptor mutations. • Visceral obesity and high BMI ( visceral adipose suppresses adiponectin secretion). • Insulin resistance and hyperinsulinemia. • Dyslipidemia (high TGs & LDL-C, low HDL-C) • Inflammation and increased risk of DM and coronary heart disease (TNG-a inhibits adiponectin.) • Stress (Symathetic stimulation reduces adiponectin.) Low Adiponectin associated with: Low Adiponectin associated with: Metabolic Markers - Adiponectin
High HOMA-IR associated with: • Hepatic insulin resistance—a result of ineffective suppression • of hepatic glucose production by insulin, declining beta-cell • function, or both. • Increased risk (or presence) of CVD and diabetes (high HOMA-IR may precede DM for several years).3 • Increased risk of hypertension, dyslipidemia, coagulation,and vascular endothelial dysfunction, even in the absence of glucose intolerance.4 Normal HOMA-IR associated with: • Optimal insulin sensitivity • Low fasting glucose or insulin, since HOMA-IR closely associates with both. Refer to glucose and insulin measurements • for pertinent information. • • Note: A false-normal HOMA-IR score may occur in DM when impaired beta-cell function causes greater secretion of pro-insulin than insulin in the fasting state. (See section for Pro-insulin). Metabolic Markers-HOMA-IR
To reduce Leptin Resistance (and Leptin): Metabolic Markers-Leptin