Download
1 / 19
210 likes | 781 Views
RADIOLOGY - CXR. Bronchiectasis - vessel ‘crowding’ - loss of vessel markings - tramline/ring shadows - cystic lesions/ air-fluid levels - evidence of TB Poor: diagnostic sensitivity monitoring of progression 3. RADIOLOGY - HRCT. - bronchial dilatation - bronchial wall thickening

E N D
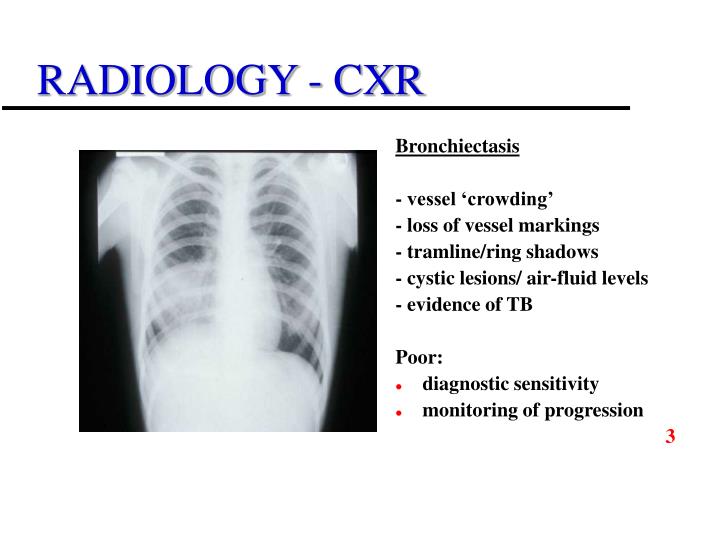
RADIOLOGY - CXR Bronchiectasis - vessel ‘crowding’ - loss of vessel markings - tramline/ring shadows - cystic lesions/ air-fluid levels - evidence of TB Poor: • diagnostic sensitivity • monitoring of progression 3
RADIOLOGY - HRCT - bronchial dilatation - bronchial wall thickening - classification (pathology) • sensitivity (97%) > CXR3 • chromosomal radiosensitivity - plain CXR (x 3 days background) - HRCT: x 30-40 - conventional CT: x 200 • ? routine baseline • ? (a)symptomatic monitoring
UNSUSPECTED DISEASE(Clinical v CXR v HRCT) • Bronchiectasis in Hypogammaglobulinaemia - A ComputedTomography assessment.Curtin et al. Clinical Radiology (1991) 44, 82-84 • Radiologic Findings of Adult primary Immunodeficiency Disorders.Obregon et al. Chest (1994)106, 490-495 • Chest High Resolution CT in Adults with Primary Humoral Immundeficiency.Feydy et al. British Journal of Radiology (1996) 69, 1108-1116 • Clinical Utility of High-Resolution Pulmonary Computed Tomography in Children with Antibody Deficiency.Manson et al. Pediatric Radiology (1997)27, 794-798 • The Value of Computed Tomography in the Diagnosis & Managementof Bronchiectasis.Pang et al. Clinical Radiology (1989) 40, 40-44 • Review Article: Imaging in Bronchiectasis.Smith et al. British Journal of Radiology (1996) 69, 589-593 3
Kainulainen et al 1999 CVID x 18, XLA x 4 CXR HRCT Bronchiectasis3 16 3 year follow-up Disease progression (5) Serum IgG Case NoT=0 T=36 1 9.9 10.0 2 4.6 6.1 8 3.7 5.1 10 3.7 4.9 21 3.1 5.7 RADIOLOGY
RADIOLOGY - HRCT RCP Specialty Specific Standards ‘Fit’ patients…….CT scanning should be undertaken in a minority of patients but usually not more than once a year or if respiratory function tests or symptoms deteriorate JCIA November 20014
MANAGEMENT – GENERAL ISSUES • Shared Care (Immunologist/Respiratory Physician) optimal 4 • Bronchodilators (reversible airflow obstruction) • Mucolytics - insufficient evidence to evaluate routine use (Cochrane Database of Systematic Reviews. 3, 2003) • Physical therapy- insufficient evidence to support or refute usage (Cochrane Database of Systematic Reviews. 3, 2003) • Anti-inflammatory agents
REPLACEMENT THERAPY • Risk/benefit assessment 4 • IV/Sc routes optimal 2 • pulmonary infections in XLA/CVID (v untreated)2 • Optimal dosing/frequency/serum IgG level not established • Tailor route/dose/infusion frequency3 --------------------------------------------------------------- • Maintain IgG >5g/l2 • Paediatric target: mid reference range4 • IgG: >8g/l infection (v 5g/l, XLA, children)3 9.4 g/l infection (v 6.5g/l, XLA/CVID, children/adults)3 • High v standard doses infections (no. & duration)2 days hospitalised serum IgG • Insidious disease progression despite ‘adequate’ replacement3
REPLACEMENT THERAPYHigh dose v low dose: secondary outcome, pulmonary function • Eijkhout et al 2001(randomised, double-blind, multicentre, crossover, n=43) High dose (mean trough IgG 9.4 g/l): PEFR 37.3 l/min Standard dose (mean trough IgG 6.5 g/l): PEFR 11.4 l/minNS • Roifman & Gelfand 1988 (ramdomised, crossover, n=12) High dose FVC & FEV1p<0.01 • Roifman et al 1987(randomised, crossover, n=12) Mean FEV1 & FVC high dose phase v low dose phasep<0.01 • Bernatowska et al 1987 (two-dose, crossover, non-randomised, n=13) High dose Max. expiratory flow & FEV1NA
ACUTE INFECTION MICROBIOLOGY • Culture & sensitivity routinely in acute setting3 • Value unclear in chronic situation - confirm original pathogen - ? emerging resistance - additional pathogens ANTIBIOTICS • Effectiveness established in exacerbations (bronchiectasis)2 • Higher doses for longer periods4 • Local treatment protocols4
ANTIBIOTIC PROPHYLAXIS • Chronic bronchitis - no place in routine treatment (Cochrane Database of Systematic Reviews. 3, 2003) • Cystic fibrosis benefits - principally staphylococci - infancy 3/6 years - ? older children/adults - ? > 3years treatment (The Cochrane Library, Oxford. 2, 2003) (Cochrane Database of Systematic Reviews. 3, 2003) • Bronchiectasis - limited meta-analysis (6 RCTs) - marginal benefit / cautious support (Evans et al. Thorax 2001)
ANTIBIOTIC PROPHYLAXIS • No robust data v placebo • No substantial data v (or additional to) IVIg/SCIg(Silk et al. 1990) • ? Single intervention in mild antibody deficiency - not in more severe phenotypes / tissue damage • Papworth protocol:consider if: > 3 exacerbations / year4 radiological / PFT deterioration • ? Eradication/clean-up therapy prior to prophylaxis - no clear evidence of benefit in antibody deficiency + structural lung damage • Development of local protocols for management of infections (esp.with Primary Care) and initiating prophylaxis4
(Heelan et al., ESID 2002) ANTIBIOTIC PROPHYLAXIS
SURGERY • Diagnostic delay > 2 years: need for surgical procedures Adequate treatment: lobectomy/pneumonectomy by 95% (UK PAD Audit 1993-96)3 • Important treatment option with favourable outcomes especially in focal bronchiectasis (Cohen et al 1994, Mansharamani & Koziel 2003)3
QUESTIONS / ISSUES • HRCT in routine screening & monitoring • Radiological changes a primary therapeutic target - Does HRCT modify our current assumptions about criteria for adequate treatment of antibody deficiency disorders? • Correct level of Ig treatment - arbitrary target serum level (evidence) or individualised (clinical + HRCT factors) - single intervention universally applicable in all patients (probably not) - higher doses: expense, complications, limited commodity • Roles of: antibiotics anti-inflammatory agents bronchodilators aids to airway clearance • Role of co-factors (e.g. 1AT) • Selective IgA deficiency
PIN GUIDELINES • Identify need for focused clinical research • Encourage debate and discussion • Reflect uncertainties in the field • Proscriptive as necessary, flexible where possible