Download
1 / 64
650 likes | 1.15k Views
CXR review. Cheryl Pirozzi MD 2010 Adapted from… Many prior CMRs. Know Your Anatomy. Normal PA CXR. Have a System. A System. Always include: Description: Always say the type of radiograph, the patient’s name and the date the study was done.

E N D
CXR review Cheryl Pirozzi MD 2010 Adapted from… Many prior CMRs
A System • Always include: • Description: Always say the type of radiograph, the patient’s name and the date the study was done. • Lines/tubes/soft tissue: This may be the reason you have a CXR, if so, comment first. • Comparison: Is this different from previous films?
A System Outside In: • Description and Big Picture • Lines and other non-human stuff • Bones and soft tissues • Lungs • Mediastinum and heart • Comparison
Another System- RIP ABCs • RIP ABC’s • Helpful for remembering what needs to be covered • Not as intuitive as other techniques
Another System- RIP ABCs • R – Rotation • I – Inspiratory Effort • P – Penetration • A – Airway • B – Bones • C – Cardiac shadow (include mediastinum) • D – Diaphragm • E – Effusions • F – Free Air • G – Gotta get to the lungs
Another System- RIP ABCs • Rotation • Examine the clavicular heads • They should be flush with the sternum • Equidistant from midline • Rotated images can change appearance of normal structures
Another System- RIP ABCs • Inspiration • Normal lung inflation 8-10 ribs • Underinflated <8 • Poor inspiration can cause a washed-out appearance to lungs, which can mimic pneumonia or effusion • Overinflated >10 • COPD, air trapping
Another System- RIP ABCs • Penetration • Over penetrated • Too dark • Under penetrated • Too bright • Ideal penetration should allow you to see the vertebrae through the cardiac silhouette.
Another System- RIP ABCs • A: Airway • Trachea midline? • If not, why?
Another System- RIP ABCs • B: Bones • Here’s you chance to shine! • Look for fractures • Follow each rib • Look at clavicles • Some ability to see shoulder and scapula
Another System- RIP ABCs • C: Cardiac shadow and mediastinum • Cardiac shadow should be less than ½ overall thoracic distance • Be careful calling it cardiomegaly
Another System- RIP ABCs • Mediastinum • Look for widened mediastinum • Widened mediastinum often denotes aortic aneurysm or mass • Anomalous mass in anterior mediastinum is usually one of the 4 T’s: • Teratoma • Thymoma • Thyroid mass • Terrible Lymphoma
Another System- RIP ABCs • D: Diaphragm • Look at level of diaphragm, right is usually higher but large differences could indicated neuromuscular problems • Comment on: • Flattening • Air underneath • Gastric bubble • Loss of the costophrenic angle • Deepening of the CPA
Another System- RIP ABCs • Effusions • How do you identify an effusion?: • CPA blunting • Meniscus • White Out!! • Often won’t see a pleural effusion unless >300 ml • Verify pleural effusion with lateral decubitus
Another System- RIP ABCs • Free air • Can be anywhere: often under diaphragm, in anterior mediastinum (pneumomediastinum) or soft tissue (abscess, crepitus)
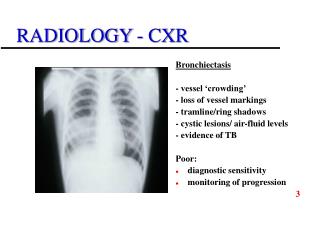
Another System- RIP ABCs • Gotta get to the lungs • Look for any pathology in lungs (as discussed) • Look at vasculature, follow it out – loss of vasculature could indicate a pneumothorax
Terminology A great rule of thumb is to remember to be descriptive. • Opacity • Consolidation, ground-glass, band-like, confluent, patchy, diffuse, wedge-shaped… • Avoid “infiltrate” – implies pneumonia • Nodule < 3 cm • Mass > 3 cm • Extrapulmonary • Best descriptive term for things outside the lungs, such as pleural, rib or soft tissue processes.
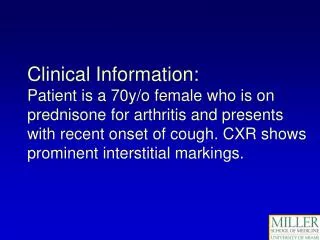
Terminology • Reticular: Usually means interstitial disease--Septal lines (Kerly B lines) • linear, curvilinear or lace-like • Alveolar Pattern • Caused by things that fill the alveoli • What fills alveoli—only 5 things • Blood • Pus • Water • Protein • Air
Radiographic Pathology • Pneumonia • Many types (lobar, segmental, bronchial, necrotizing, etc.) • Many etiologies (aspiration, bacterial, viral, fungal, etc.) • Infiltration or consolidation? Just use opacification
RadiographicPathology • Silhouette Sign • Helps determine location of opacification
Radiographic Pathology • Pleural Effusions • Something between visceral and parietal pleura (blood, fluid, pus) • Costophrenic angle blunting • Look for meniscus • Can only be seen on CXR when it exceeds 300 ml.
Radiographic Pathology • Right Lateral Decubitus
Radiographic Pathology • Masses • Tumors • Lymph nodes • Aspirates/foreign bodies
Radiographic Pathology • Disruption of continuity • Fractures
Radiographic Pathology • Spacing/location/ relative size • Widened mediastinum • Tracheal shift • Cardiomegaly
CASE #1 – Two weeks later Acute Shortness of Breath
CASE #5 Post- procedure