Download
1 / 38
650 likes | 2.2k Views
NEISSERIA GONORRHOEAE. Albert Ludwig Sigesmund Neisser. Albert Ludwig Sigesmund Neisser was a German physician who specialized in dermatology and venereal diseases. He discovered gonococcus (1879), the small bacterium that causes gonorrhoea. Gonorrhea.

E N D
Albert Ludwig Sigesmund Neisser • Albert Ludwig Sigesmund Neisser was a German physician who specialized in dermatology and venereal diseases. • He discovered gonococcus (1879), the small bacterium that causes gonorrhoea.
Gonorrhea • The name Gonorrhea is derived from Greek words- Gonos ( seed ) rhoia ( flow ) • Describes a condition in which semen flowed from the male organ without erection,
Gonorrhea – Venereal Disease • Gonorrhea is a classical venereal disease, being spread almost exclusively by sexaul contact having a short incubation period and being relatively easy to diagnose and treat.
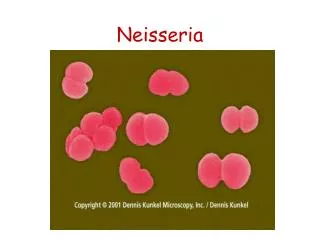
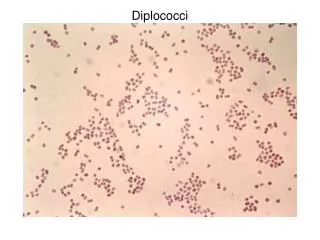
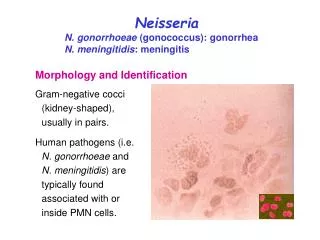
Neisseria gonorrhea • Neisseria gonorrhea are gram negative oval cocci with opposing surfaces slightly concave ( Bean shaped )
Neisseria gonorrhea • Neisseria species are Gram-negative cocci, 0.6 to 1.0 µm in diameter. • The organisms are usually seen in pairs with the adjacent sides flattened. • Pili, hairlike filamentous appendages extend several micrometers from the cell surface. • The outer membrane is composed of proteins, phospholipids, and Lipopolysacchride (LPS)
N.gonnorhea infects mucous membrane • Gram-negative intracellular diplococci of the species Neisseria gonorrhoea, the cause of gonorrhoea; • a nonmotile aerobic microorganism of the species N. gonorrhoea. • It is a parasite of the mucous membrane.
Pathogenesis • N.gonnorhea is Human pathogen. • Chimpanges can be infected artificially • Women may remain Asymptomatic • Gonorrhea infection is generally limited to superficial mucosal surfaces lined by columnar epithelium.
The Organs and Tissues involved • Cervix • Urethra • Rectum • Pharynx • Conjunctiva • Vaginal epithelium – covered with Squamous epithelium not infected • However prepubertal vaginal epithelium is infected in young girls present with vulvovaginitis
Pathogenesis ( contd ) • Gonorrhea is Venereal disease • The disease is acquired by sexaul contact. • In general incubation is 2 -8 days • In men the disease starts as purulent discharge containing gonococci in large numbers. • The disease spreads to prostate, seminal vesicle, and epididymis • In men chronic urethritis may lead to stricture formation
Clinical Presentation in Males • Majority of males present with acute Urethritis with purulent discharge • 5% of patients carry bacteria without distress • Rectal and Pharyngeal infections are less often symptomatic
Clinical Presentation in Females • Endocervix infection is the most common presentation in women • Present with vaginal discharge and Dysuria • Infection and abscess of Bartholin and Skene’s glands
Complications of GC Infections in Women • Infertility • Ectopic Pregnancy • Chronic Pelvic Pain • Psychosocial Upper Tract Infection Local Invasion Systemic Infection Genital Infection Congenital Infection HIV Infection
Other Manifestations • Rectal infection (Proctitis) with N.gonnorhea occurs one third of women with cervical infection. • Rarely symptomatic. • Acute salphingits • Pelvic inflammatory disease • Sterility
Other Manifestations • Peritonitis can spread • Fitz Hugh Curtis Syndrome. • Disseminated gonococcus infection • Painful Joints may lead to Arthritis • Fever, Few septic lesions on the extremities • Meingitis and Endocarditis
Gonococcal Opthalmia • Babies born to infected women suffer, can lead to a serious condition of Opthalmia neonatroum • Manifest with sever purulent discharge with periorbital edema within a few days of birth • Topical application of 1% silver nitrate has drastically reduced the incidence. • In present contest Topical erythromycin is used.
Gonococcal infection in Prepubertal Girls • Vulvo-vaginitis in prepubertal girls occur in conditions of poor hygiene or by sexual abuse • All cases to be investigated with care and caution.
Disseminated Infections • Seen more commonly in women who may present with painful joints, fever, and few septic lesions or the extremities • Rarely disseminated infections may present as Endocarditis or meningitis.
Laboratory Diagnosis • Specimens are collected with care and caution. • Specimens are collected from sites with scanty commensals eg Endocervix
Transportation of Specimens • It is preferred in culture, specimens should be inoculated in prewarmed plates, immediately on collection • If not possible specimen should be collected on charcoal impregnated swabs and sent to laboratory in Stuart’s transport medium.
GC Diagnostic Methods • Gram stain smear • Culture • Antigen Detection Tests: EIA & DFA • Nucleic Acid Detection Tests • Probe Hybridization • Nucleic Acid Amplification Tests (NAATs) • Hybrid Capture
Gram stain (male urethra exudate) DNA probe Culture NAATs * Sensitivity 90-95% 85-90% 80-95% 90-95% Gonorrhea Diagnostic Tests Specificity >95% >95% >99% 98% * Able to use URINE specimens
Gram Staining • Gram’s method of staining is sensitive in 95% of infections. • The demonstration of intracellular Gram negative intracellular diplococci in stained smears provides a presumptive evidence of gonorrhea in men. • Specimens are inoculated onto culture plates freshly prepared. • Delay in inoculation of specimens on culture media reduces the rate of isolation.
Culturing Gonococci • Gonococci are aerobic and may grow aerobically • It is essential to provide 5 – 10% CO2 • They grow well on Chocolate agar and Mueller – Hinton agar • The colonies are small, convex, translucent, and slightly umbonate, with finely granular surface and lobate margins.
Selective Culture Medium • The selective medium is Thayer – Martin medium containing Vancomycin, colistin, and Nystatin, effectively inhibits most contaminants including non pathogenic Neisseria
Culturing is possible in specialized diagnostic laboratories only. • The combination of Oxidase positivecolonies andGram negative diplococci provides a presumptive diagnosis.
Fluorescent Methods • Florescent methods will help in prompt detection in infected patients • Various discharges can be examined.
Other Methods in Diagnosis • Co agglutination methods • Biochemical tests to differentiate from other commensals resembling Neisseria spp
Treatment • Penicillin was a popularly used antibiotic. However resistance has reduced it utility. • For a long time the drug resistance has overcome with increased dosage • Complete resistance to penicillin has made the drug obsolete in several parts of the world.
Genes Code resistance • The penicillin resistant strains possess the gene coding for TEM-type ß-lactamase commonly found Escherichia coli
Other Drugs in current use • Ceftriaxone • Cefixime • Fluoroquinolones • Ciprofloxacin • Tetracycline • Co- Amoxiclav • Spectinomycin In Disseminated Gonococcal disease and any complicated infection treatment for 7-10 days is necessary
Controlling Gonorrhea • The key control measures in gonorrhea are 1 Rapid diagnosis 2 Use of effective antibiotics 3 Tracing, examination and treatment of contacts. 4 Inappropriate self medication has contributed to widespread antimicrobial resistance.
NON-GONOCOCCAL URETHRITIS • Chronic urethritis where gonococci cannot be demonstrated. • Can be considered as non-specific urethritis. • Urethritis forms part of the syndrome consisting of conjunctivitis and arthritis (Reiter's syndrome). • May be also due to Gonococcal infection, the cocci persisting as l-forms and hence undetectable by routine tests.
CAUSATIVE AGENTS: • Chlamydia trachomatis • Ureaplasma urelyticum. • Mycoplasma hominis. • Herpes virus • Cytomegalo virus. • Trichomonas vaginalis. • Candida albicans. • Can also be due to mechanical or chemical irritation. • Management: difficult.