Download
1 / 1
10 likes | 110 Views
Use of Safe-laser Technology to Train Head Movement in Locked-In-Syndrome. Susan K. Fager MS CCC-SLP 1,2 , David R. Beukelman Ph.D. 1,2 , Renee Karantounis MS CCC-SLP 3 , Tom Jakobs P.E. 4 1 Institute for Rehabilitation Science and Engineering at Madonna Rehabilitation Hospital

E N D
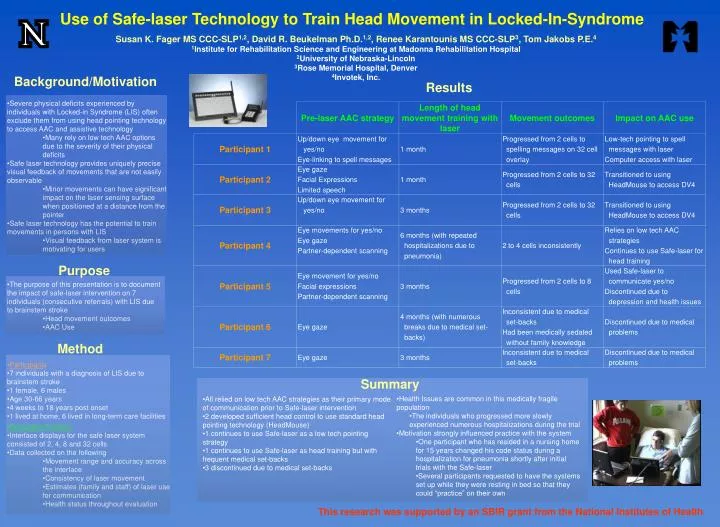
Use of Safe-laser Technology to Train Head Movement in Locked-In-Syndrome Susan K. Fager MS CCC-SLP1,2, David R. Beukelman Ph.D.1,2, Renee Karantounis MS CCC-SLP3, Tom Jakobs P.E.4 1Institute for Rehabilitation Science and Engineering at Madonna Rehabilitation Hospital 2University of Nebraska-Lincoln 3Rose Memorial Hospital, Denver 4Invotek, Inc. Background/Motivation Results • Severe physical deficits experienced by individuals with Locked-in Syndrome (LIS) often exclude them from using head pointing technology to access AAC and assistive technology • Many rely on low tech AAC options due to the severity of their physical deficits • Safe laser technology provides uniquely precise visual feedback of movements that are not easily observable • Minor movements can have significant impact on the laser sensing surface when positioned at a distance from the pointer • Safe laser technology has the potential to train movements in persons with LIS • Visual feedback from laser system is motivating for users Purpose • The purpose of this presentation is to document the impact of safe-laser intervention on 7 individuals (consecutive referrals) with LIS due to brainstem stroke • Head movement outcomes • AAC Use Method • Participants • 7 individuals with a diagnosis of LIS due to brainstem stroke • 1 female, 6 males • Age 30-66 years • 4 weeks to 18 years post onset • 1 lived at home, 6 lived in long-term care facilities Summary • Health Issues are common in this medically fragile population • The individuals who progressed more slowly experienced numerous hospitalizations during the trial • Motivation strongly influenced practice with the system • One participant who has resided in a nursing home for 15 years changed his code status during a hospitalization for pneumonia shortly after initial trials with the Safe-laser • Several participants requested to have the systems set up while they were resting in bed so that they could “practice” on their own • All relied on low tech AAC strategies as their primary mode of communication prior to Safe-laser intervention • 2 developed sufficient head control to use standard head pointing technology (HeadMouse) • 1 continues to use Safe-laser as a low tech pointing strategy • 1 continues to use Safe-laser as head training but with frequent medical set-backs • 3 discontinued due to medical set-backs • Evaluation Protocol • Interface displays for the safe laser system consisted of 2, 4, 8 and 32 cells • Data collected on the following • Movement range and accuracy across the interface • Consistency of laser movement • Estimates (family and staff) of laser use for communication • Health status throughout evaluation This research was supported by an SBIR grant from the National Institutes of Health