Download
1 / 37
420 likes | 797 Views
Management of Testicular GCT . By Dr.Turky Al- Mouhissen Chief Urology Resident – WR R5 Urology – KKNGH. Relapse 17%, median 15/12, O.S. 98%. Recurrence rate 9%. 15-20% of stage 1 will have retroperitoneal L.N. disease. 25 Gy 5yr SR >95% Dogleg Paraortic Strip. 30-35 Gy

E N D
Management of Testicular GCT By Dr.Turky Al-Mouhissen Chief Urology Resident – WR R5 Urology – KKNGH
Relapse 17%, median 15/12, O.S. 98% Recurrence rate 9% 15-20% of stage 1 will have retroperitoneal L.N. disease 25 Gy 5yr SR >95% Dogleg Paraortic Strip
30-35 Gy 5y surv. 80%
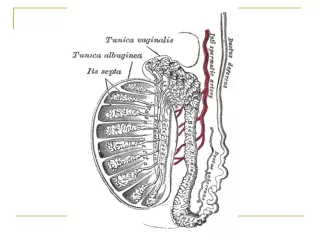
Sheet of tissue Around great vessels 27%
Residual mass post chemo. : • 27 % Seminoma: >3cm, well discrete Excision • 10-19% Nonseminoma: low threshold for surgical excision, combined with RPLND Surgical excision in Nonseminoma can be avoided if: >90% response of tumor to chemo. With absence of teratoma in primary tumor
Nonseminomatous Germ Cell tumors Relapse rate 28% >60% in Retroperi. If Relapsed chemo / pN2 20-25% clinical stage 1 is understaged In stage 1, 30% have Retroperi. disease 5-10% relapse
Back pain • Contralateral / multifocal disease • High tumor markers • Suprahilar L.N. 48% Relapse rate
International germ cell classification system for testicular ca.
(Good & Intermediate Risks) Response rate 90-95% 20% disease free Post salvage chemo residual mass: 50% Ca. 40% Teratoma 10% fobrosis Response rate 50% Residual mass post therapeutic chemo: 10% Ca., 50% Teratoma, 40% Fibrosis
Rt side: • Interaortocaval, preaortic & precaval, paracaval, Rt iliac • Lt side: • Paraortic, preaortic, interaortocaval, Lt iliac
B/L RPLND • Transabdominal approach • 2-3 hours procedure • Negligible mortality, morbidity 5-25% • Morbidity related to : • Atelactasis • Pneumonitis • Ileus • Lymphocele • pancreatitis
Long term morbidity of B/L RPLND: • Loss of antigrade ejaculation • infertility
Modified (Template) RPLND Interaortocaval & Ipsiplateral L.N. betw. Renal vessels & bifurcation of Common Iliac artery Avoid contralateral dissection below IMA Time consuming Require steeper learning curve Ejaculation preserved in 100% Fertility noted in 75%
lymphadenectomy • Dissection of renal veins to the IVC • Gonadal vessels ligated • Tributaries of Renal vein in left side ligated • Adrenal • Gonadal • Lumbar • Anterior split on the surfae of the aorta is done inferiorly to the level of the bifurcation of iliac art.
Renal art. Skeletonized • Gonadal art. Ligated to prevent subadventetialhemtoma if they are avulsed • After completing B/L dissection: • Aorta. IVC, Renal vessels should be skeletonized • Ant. Spinouslig. Visible • Stumps of Rt. & Lt. gonadal vessels & IMA are visible • Irrigation with warm water • Lymphostasis & hemostasis secured
Post. Parietal peritoneum loosly approx. • Fascia closed • Postoperative tachycardia is common due to sympathaticdishcarge
Scrotal violation • Suboptimal approaches to testicular neoplasms • 4-17% • Scrotal orchiectomy • Transscrotal biopsy • Fine-needle aspiration
A recent metaanalysis of 206 pts reported • local recurrence rate 2.9% compared to 0.4% treated with inguinal approach • no difference in systemic relapse or survival rate • No advantage to adjuvant chemo. (capelouto et al 1995)
Recommendations for pts with scrotal violation : • In low stage seminoma, radiation portals should include ipsilateral groin & scrotum • Low stage NSGCT, scrotal scar should be widely excised with spermatic cord remnant at the time of RPLND • Pts with clinical stage 1 NSGCT & scrotal violation are not good candidates for surveillance • Pts treated with full dose platinum based regimen should have the cord stump removed at RPLND • Extensive groin dissection / hemiscrotectomy not required due absence of local relapse after systemic treatment
Note: Pts with h/o herniorrhaphy / prior orchidopexy in stage 1-2 seminoma, should have contralateral inguinal region to be irradiated with contralateral testicle shielded
chemotherapy • Adjuvant / Therapeutic Chemo. is BEP= bleomycin + Etoposide + Cisplatin • 3 cycles of BEP = 4 cycles EP in Therapeutic Chemo. • Salvage Chemo. is VIP= Vinblastine + Ifosfamide + Cisplatin
S/E: • Bleomycin: Skin toxicity • Most frequent S/E, reported approximately 50% of treated patients • Erythema, rash, striae, vesiculation, hyperpigmentation, skin tenderness • Hyperkeratosis, nail changes, alopecia, pruritus, and stomatitis, scleroderma • Usually late, occurs at 2nd and 3rd week of treatment Pulmonary fibrosis Hypersensitivity reaction CVS S/E such as MI, CVA, Thrombotic events Gastrointistinal S/E (Rare)
Bleomycin Pulmonary Toxicty (BPT) : • Occurs in 6.8% • Mortality rate 1% • Risks • >40 year old • GFR<80 • Advanced • Cumulative dose effect • Rx • Keep hypovolemia • Keep low Fi O2
Etoposide: Secondary leukemia (dose dependent) Alopecia Myelodepression Mild renal impairment • Cisplatin: Nephrotoxicity Neurotoxicity Ototoxicity Nausea & vomitting
Vinblastine: Generally not lasting more than 24 hours Leukopenia, myelosuppression Alopecia Gastrointestinal symptoms Parasthesia • Ifosfamide: Hrgiccysitis (should use Mesna before it to prevent it) Mild renal insuffeciency (usually transient), 4-7% Myelosuppression