Download
1 / 12
120 likes | 161 Views
Detailed case study of a 27-year-old male with ARN induced by VZV, treatment, and outcomes. Importance of early intervention and combination therapy discussed.

E N D
Dr. Rathinam Sivakumar HOD - Uveitis Services Dr. Radhika. T Consultant, Uveitis Service Dr. Vedhanayaki Rajesh Consultant, Uveitis Service Acute Retinal Necrosis
OcularHistory 27 yearold male OD: defectivevision, painandredness since 15 days nospecificsystemicillness
First Presentation VA: OD 6/36, OS 6/6 IOP: OD 18mm Hg; OS 18mm Hgby NCT OD: granulomatousKP's on endothelium AC 3+ cells; flare 2+ AVF 3+ cells; retinalnecrosis with sclerosedvessel OS: quieteye
First Presentation – Lab Findngs Routine baselineinvestigationswereperformedandwerewithin normal limits HIV Tridot -ve Vit. Tap : PCR +vefor VZV
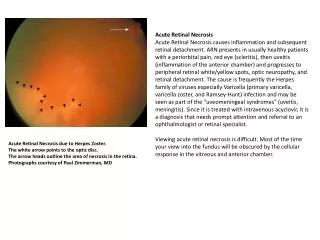
Diagnosis Acuteretinalnecrosis inducedbyvaricella-zoster virus
Treatment steroid with antibiotics e/d – taperingtherapy homatropine e/d twice/day – 1 week Topicalganciclovir gel 3x/day oral valacyclovir 1gm 3x/day oral prednisolonetaperedweeklyfrom 40 mg/ weekto 10mg (4 weeks) intravitreal gancyclovir (2mg / 0.1 ml)
Second Presentation – After 3 weeks VA: OD 6/9, OS 6/6 IOP: OD 10mm Hg; OS 18mm Hgby NCT OD: AC quiet; HealingRetinalnecrosis OS: Quieteye Patient was continued on oral valacyclovir
Third Presentation – After oneMonth VA: OD 5/60, OS 6/6 OD: AC – Occ. Cells fundus: retinaldetachment (post ARN) pars plana vitrectomy +/- membranepeeling + endolaser + siliconeoilimplantation continued on oral valacyclovir
Final Presentation – After 1 Month BCVA: OD 6/9, OS 6/6 OD: AC – Quiet Fundus: siliconeoilfilledglobe settledretinaldetachment
Conclusion • ARN ischaracterisedbyacuteperipheralnecrotisingretinitis, retinal arteriolitis with severe vitritis • Itcanbecausedby VZV / HSV in both immunocompetent andcompromisedpatients • Retinitis progressesrapidly in theabsenceoftreatment. Rhegmatogenous retinaldetachmentcanoccurfromatrophicareaspostretinalnecrosis • Intravitreal Gancyclovirand oral antiviral therapyarethebesttreatmentoptions. Corticosteroidsareinitiated with anti-virals in taperingregimen