Download
1 / 34
390 likes | 727 Views
Neuroanatomy. Hathaway Fiocchi July, 2010. Study Tips. Course objectives Power points Handbook Anatomy 1 powerpoints to review the basics In Dr. G’s folder: “Nervous System (2 lectures)” Make sure to go over Dr. Lannings ppts because she added some stuff! . Intro to Neurobio.

E N D
Neuroanatomy Hathaway Fiocchi July, 2010
Study Tips • Course objectives • Power points • Handbook • Anatomy 1 powerpoints to review the basics • In Dr. G’s folder: “Nervous System (2 lectures)” • Make sure to go over Dr. Lanningsppts because she added some stuff!
Intro to Neurobio • What is the point of all this? • Neuroanatomic diagnosis • Two questions to answer in this course: • Is the nervous system involved in producing the observed dysfunction? • Where is the nervous system damaged? = neuroanatomic diagnosis
Blood supply to the brain • Circle of Willis • Vertebral aa. contribute to 1 Basilar a. • Internal Carotid aa. (2) • ReteMirabile • When you don’t have major blood supply from the internal carotid • Cow, Cat, Pig Blood supply to the spinal cord • 1 ventral spinal a. • 2 Dorsal spinal aa.
Meninges • 3 layers: • Dura mater • Most external • Thickest • Well innervated • Falxcerebri • Arachnoid: • Middle layer • Arachnoidtrabeculae • Arachnoid granulations: CSF drainage • Pia mater: • Innermost, closely adhered to the nervous tissue • Highly vascular • Assoc. with denticulate ligament of the spinal cord
Spaces • Epidural space • Mainly potential space in brain • Fat and vessel filled space in spinal cord • Used for injections • Subdural space • Potential space in both brain and spinal cord • Subarachnoid space • Interdigitated with arachnoidtrabeculae • Contains CSF • Sites in the brain for tapping and sites on spinal cord
Meninges Cranial vs. Caudal • Pia mater is same in the brain and spinal cord • Arachnoid • Specialized enlarged areas around the brain = cisterns • Cerebellomedullary cistern is preferred site for CSF collection in small animals and in large animals under anesthesia • Dura Mater • Outer and inner layer of the dura are closely adhered • NO epidural space around the brain = potential space • Big epidural space in the spinal cord = injections • Dural reflections compartmentalize the brain and reduce movement • falxcerebri: midline of the cerebrum
Cranial Meninges and Spaces 3 Layers 3 Spaces
Spinal Meninges Pia Mater Dura Mater Arachnoid Where does an Epidural go?
Caudal Meninges • Filumterminale: Terminus of the spinal cord • Caudal ligament: Attachment of filumterminale to last vertebral foramen • Lumbospinal cistern: for CSF tap in caudal meninges-in the subarachnoid space around the filumterminale • Epidural space is full of fat and vessels and can be used for injections--carefully! Can you label the: Dura, Arachnoid, Pia, Filumterminale, Caudal ligament and Lumbospinal Cistern?
Meninges and Spaces con’t. • What space is used for collection of CSF? • Subarachniod space • What space is used for injections? • Epidural space In both cranial and caudal meninges? No, caudal only—why?
CSF production, drainage • CSF: is an ultrafiltrate of blood • Produced by: ependymal cells of the choroid plexuses within the ventricles • Drained by: arachnoid granulations—one way valve system moves CSF into dural sinuses • Dural sinuses are valve-less system • Functions • Water-jacket • Lymphatics • Transport hypothalamic hormones within brain • CO2 concentration monitoring
Ventricles • Vestiges of the neural tube within the brain tissue and spinal cord • Lined with special glial cells called ependymal cells of the choroid plexuses which help produce and circulate the CSF within the ventricles • Ventricles all connected and CSF flows from cranial to caudal until the 4th ventricle • Flow of CSF through the ventricles: Lateral 3rd 4th arachnoid space (meninges) or central canal
Ventricles Try to superimpose these 2 views in your head to understand the relationship of the ventricles in the brain
Regeneration of nervous tissue • Damage to the cell body = death • Except: olfactory neurons which regenerate! • Damage to axons of the CNS = minimal regeneration at best • Damage to axons of the PNS = more success • To muscles and viscera! • 3 types of injury to an axon • Stretch related • Lacerations • Compression (mechanical or vascular) • Extent of regeneration depends on the number and severity of axons damaged
Which of the following injuries has the best chance of regeneration? • Damage to axon in CNS • Damage to cell body in CNS • Damage to axon in PNS
Parietal Lobe Occipital Lobe Frontal Lobe Cerebellum Temporal Lobe Brain Stem Olfactory bulb Pyriform Lobe Optic Nerve
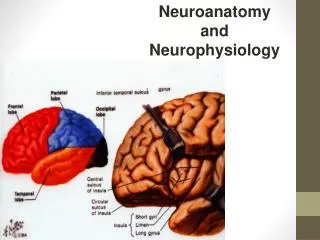
Cerebrum Highest function of the CNS • Seat of consciousness and cognitive functions • Receives all sensory information that reaches conscious perception—not reflexes! • Divided into 2 hemispheres: left and right • Each hemisphere has 5 lobes
Occipital lobe: - Perception of visual stimuli - Damage causes cortical blindness - Reflex arcs are still intact 5 Lobes of the Cerebral Cortex • Parietal lobe: • Perception of sensory information to create a 3D map of the world/body in space • Damage causes hemineglect Parietal Lobe Occipital Lobe Frontal Lobe Temporal Lobe • Temporal lobe: • Processing of hearing • Input from each ear goes to BOTH left and right temporal lobe • MOST is contralateral • Damage to one lobe does NOT result in deafness even in just one ear • Frontal Lobe • Contains the sensory and motor cortices • Initiation of movement • Damage manifests in a delay of initiating movement or inappropriate initiation • Lesion is contralateral to the side of manifestation Pyriform Lobe • Pyriform Lobe: • - Perception of olfaction • Associated with the Limbic system • Complete damage is Anosmia
Cerebrum: Major functions • Sensory input • Olfaction to pyriform • (olfactory bulbs are technically considered part of the pyriform lobe) • Auditory to temporal lobe • Vision to occipital lobe • Frontoparietal region for contralateralsomatosensoryinput • Somatic sensation = the senses of touch, pressure, pain, temperature • Association cortex: cognition and decision making • Motor output from the motor cortex in the frontal lobe
Damage to Cerebrum • Clinical signs of Cerebrum dysfunction • Disturbances of consciousness • Paresis of voluntary movement • What is paresis? • Disturbances of sensory function, perception and seizures
Limbic System • Limbic “Lobe” is a collection of cortical and subcortical structures functionally linked by their role in emotion and survival drives. • What is a collection of cell bodies in the CNS called? • What is a collection of cell bodies in the PNS called? • Nuclei involved in the limbic system • Hippocampus • Cingulategyrus • Hypothalamus • Amygdala • Parts of thalamus
Limbic structures • All components of the limbic system assign emotional and autonomic responses to sensory experiences • Hypothalamus – regulates autonomic functions and basic survival behaviors • Hunger, Satiety, Thirst, Temp, Osmoregulation, Circadian rhythms • Amygdala – emotional memory formation; short term • Assigning a fear response to a noxious stimuli • Hippocampus – converts short term memory to long term memory
*****ARAS**** • Maintains consciousness! • Receives collaterals from all sensory input and dictates the level of arousal in the cerebral cortex • Shapes selective attentions • Pressure on hindbrain causes most common loss of consciousness • Early compression miosis • Increased compression mydriasis • Canine Narcolepsy could be from a receptor mutation here that decreases excitatory inputs from ARAS which would normally maintain consciousness • What else comes from the hindbrain????
ARAS VOCAB • BAR: Bright Alert Responsive • Input from the cerebrum keeps you “awake” • ALERT: normal response to environmental stimuli • OBTUNDED: Withdrawn and unwilling to perform normally • DEMENTED: Animal is responsive, but the responses are abnormal • STUPOROUS: Patient unresponsive except to noxious stimuli • COMATOSE: Patient unresponsive to both environmental and noxious stimuli Oink! Are you obtunded?
Seizure • A seizures is a cortical event characterized by abnormal neuronal discharge that is both excessive and hypersynchronized • Can be caused by both excessive excitation or decreased inhibition
Stages of Seizures • Prodrome (see Lanning’s ppt): early indicator of disorder • Aura: period of altered behavior • Ictus: synchronized, hyperactive firing of neurons is occurring • Associated with a loss of consciousness • Alterations of sensation: hallucinations • Disturbances of autonomic function: salivation, tachycardia • Alterations of muscle tone associated with involuntary movements • Post-ictus: period of confusion and restlessness • Inter ictus (see Lanning’s ppt) periords between seizures
Seizure vocab • Primary Focus: restricted area of the cortex when the seizure begins • Kindling: spreading or reinforcement of the tendency to seize • Mirror focus is when seizure spreads to the contralateral side across the corpus callosum by commissural fibers
Seizure vocab • Focal seizure or partial seizure: the seizure is confined to one part of the cerebrum, there are no convulsions • Focal motor seizure = chewing-gum fit • Focal seizure with secondary generalization: neurons outside the focus are recruited • Usually within the limbic system • Produces behavioral or emotional seizures • Simple-partial seizure = term for seizure that does not affect consciousness
Seizure vocab • Generalized seizure: spreads rapidly to both hemispheres, can have convulsions with loss of consciousness • Petit mal = no convulsions • Seizures with convulsions and loss of consciousness: • Grand mal AKA tonic-clonic AKA major motor • Ictus is collapse, extensor rigidity, opisthotonus, apnea all characteristics of the tonic phase • Clonic phase: period of alternation between flexion and extension of the limbs with violent chewing or vocalization • “Paddling” • Increased autonomic = salivation, urination, defecation can also occur
Cranial Nerve Review Which cranial nerves have Parasympathetic innervation? What cranial nerves are tested with the gag reflex? What cranial nerve can regenerate its cell bodies? III, VII, IX, X IX and X I