Download
1 / 1

E N D
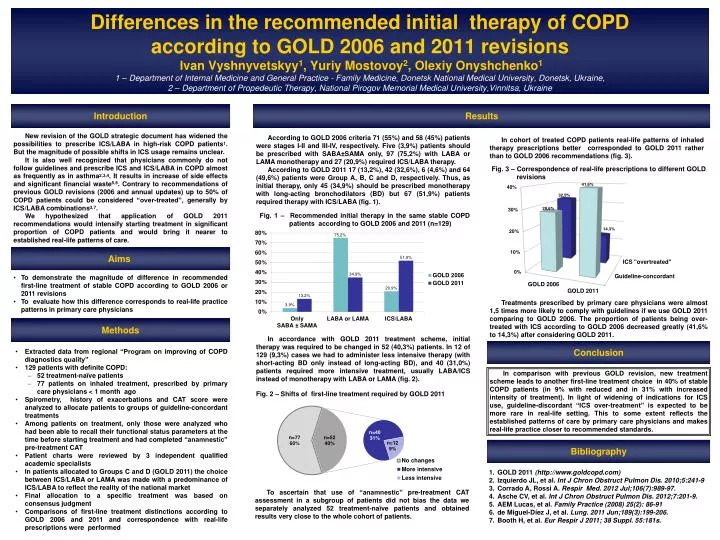
Differences in the recommended initial therapy of COPDaccording to GOLD 2006 and 2011 revisionsIvan Vyshnyvetskyy1, Yuriy Mostovoy2, Olexiy Onyshchenko11 – Department of Internal Medicine and General Practice - Family Medicine, Donetsk National Medical University, Donetsk, Ukraine,2 – Department of Propedeutic Therapy, National Pirogov Memorial Medical University,Vinnitsa, Ukraine Introduction Results New revision of the GOLD strategic document has widened the possibilities to prescribe ICS/LABA in high-risk COPD patients1. But the magnitude of possible shifts in ICS usage remains unclear. It is also well recognized that physicians commonly do not follow guidelines and prescribe ICS and ICS/LABA in COPD almost as frequently as in asthma2,3,4. It results in increase of side effects and significant financial waste5,6. Contrary to recommendations of previous GOLD revisions (2006 and annual updates) up to 50% of COPD patients could be considered “over-treated”, generally by ICS/LABA combinations3,7. We hypothesized that application of GOLD 2011 recommendations would intensify starting treatment in significant proportion of COPD patients and would bring it nearer to established real-life patterns of care. According to GOLD 2006 criteria 71 (55%) and 58 (45%) patients were stages I-II and III-IV, respectively. Five (3,9%) patients should be prescribed with SABA±SAMA only, 97 (75,2%) with LABA or LAMA monotherapy and 27 (20,9%) required ICS/LABA therapy. According to GOLD 2011 17 (13,2%), 42 (32,6%), 6 (4,6%) and 64 (49,6%) patients were Group A, B, C and D, respectively. Thus, as initial therapy, only 45 (34,9%) should be prescribed monotherapywith long-acting bronchodilators (BD) but 67 (51,9%) patients required therapy with ICS/LABA (fig. 1). In cohort of treated COPD patients real-life patterns of inhaled therapy prescriptions better corresponded to GOLD 2011 rather than to GOLD 2006 recommendations (fig. 3). Fig. 3 – Correspondence of real-life prescriptions to different GOLD revisions Fig. 1 – Recommended initial therapy in the same stable COPD patients according to GOLD 2006 and 2011 (n=129) Aims • To demonstrate the magnitude of difference in recommended first-line treatment of stable COPD according to GOLD 2006 or 2011 revisions • To evaluate how this difference corresponds to real-life practice patterns in primary care physicians Treatments prescribed by primary care physicians were almost 1,5 times more likely to comply with guidelines if we use GOLD 2011 comparing to GOLD 2006. The proportion of patients being over-treated with ICS according to GOLD 2006 decreased greatly (41,6% to 14,3%) after considering GOLD 2011. Methods In accordance with GOLD 2011 treatment scheme, initial therapy was required to be changed in 52 (40,3%) patients. In 12 of 129 (9,3%) cases we had to administer less intensive therapy (with short-acting BD only instead of long-acting BD), and 40 (31,0%) patients required more intensive treatment, usually LABA/ICS instead of monotherapy with LABA or LAMA (fig. 2). Conclusion • Extracted data from regional “Program on improving of COPD diagnostics quality” • 129 patients with definite COPD: • 52 treatment-naïve patients • 77 patients on inhaled treatment, prescribed by primary care physicians < 1 month ago • Spirometry, history of exacerbations and CAT score were analyzed to allocate patients to groups of guideline-concordant treatments • Among patients on treatment, only those were analyzed who had been able to recall their functional status parameters at the time before starting treatment and had completed “anamnestic” pre-treatment CAT • Patient charts were reviewed by 3 independent qualified academic specialists • In patients allocated to Groups C and D (GOLD 2011) the choice between ICS/LABA or LAMA was made with a predominance of ICS/LABA to reflect the reality of the national market • Final allocation to a specific treatment was based on consensus judgment • Comparisons of first-line treatment distinctions according to GOLD 2006 and 2011 and correspondence with real-life prescriptions were performed In comparison with previous GOLD revision, new treatment scheme leads to another first-line treatment choice in 40% of stable COPD patients (in 9% with reduced and in 31% with increased intensity of treatment). In light of widening of indications for ICS use, guideline-discordant “ICS over-treatment” is expected to be more rare in real-life setting. This to some extent reflects the established patterns of care by primary care physicians and makes real-life practice closer to recommended standards. Fig. 2 – Shifts of first-line treatment required by GOLD 2011 Bibliography GOLD 2011(http://www.goldcopd.com) IzquierdoJL, et al. IntJ Chron Obstruct Pulmon Dis. 2010;5:241-9 Corrado A, Rossi A. Respir Med. 2012 Jul;106(7):989-97. Asche CV, et al.Int J Chron Obstruct Pulmon Dis. 2012;7:201-9. AEM Lucas, et al. Family Practice (2008) 25(2): 86-91 de Miguel-Díez J, et al. Lung. 2011 Jun;189(3):199-206. Booth H, et al. EurRespir J 2011; 38 Suppl. 55:181s. To ascertain that use of “anamnestic” pre-treatment CAT assessment in a subgroup of patients did not bias the data we separately analyzed 52 treatment-naïve patients and obtained results very close to the whole cohort of patients.






















