Download
1 / 46
460 likes | 677 Views
Is Primary Angioplasty Equally Effective in Both Men and Women ? . Keith Dawkins MD FRCP FACC Southampton University Hospital UK. Conflicts of Interest. Research Grant Support Boston Scientific Corporation Advisory Board/Consultant Abbott Vascular Boston Scientific Corporation

E N D
Is Primary Angioplasty Equally Effective in Both Men and Women ? Keith Dawkins MD FRCP FACC Southampton University Hospital UK
Conflicts of Interest • Research Grant Support • Boston Scientific Corporation • Advisory Board/Consultant • Abbott Vascular • Boston Scientific Corporation • Conor Medsystems • Eli Lilly • Medtronic • Nycomed
Women in CardiologyEngland, Wales & N. Ireland (RCP Census) Consultant Cardiologists (n) Heart 2005;91:283-289
Establish mentors for women in cardiology • Encourage flexible training • Establish more part-time posts • Improve access for women to popular specialities (e.g. coronary intervention) • Refuse to tolerate sexism or gender based discrimination in the work place
Old Eur Heart J 2000;21:1135-1140
Women are poorly represented in cardiology • Women with cardiac disease are under investigated and under treated • Most cardiologists are men • All men are bastards… Are we following the flock…?
Injuries & Poisoning (3%) Respiratory Disease (14%) All Other Causes (22%) Other Ca (14%) Colorectal Ca (2%) Breast Ca (4%) CHD (15%) Lung Ca (4%) Other CVD (9%) CVA (12%) Deaths by Cause (Women) 2004 Office of National Statistics (2005) Scotland General Register Office (2005) Northern Ireland General Register Office (2005)
UK Glasgow UK Belfast 0 50 100 150 200 250 300 Coronary Events/100,000 population Age-Standardised Coronary Events (Women 35-64 yrs) MONICA Project Lancet 1999;353:1547-1557
Acute Myocardial Infarction (ISIS-3) p<0.001 Percent (%) Age at Presentation NEJM 1998;338:8-14
AMI: Cumulative Mortality (Day 0-35) 15 - 10 - 5 - 0 - 14.8% Women (n=6,600) 9.1% Mortality (%) Men (n=26,480) CI: 1.73 [1.61-1.86] 0 7 14 21 28 35 Days after Study Entry NEJM 1998;338:8-14
Complications of acute myocardial infarction Papillary Muscle Rupture VSD LV Rupture
Infarct Vessel Patency and MortalityGUSTO-I angiographic trial Mortality at 30 days (%) TIMI-0 TIMI-1 TIMI-2 TIMI-3 Infarct vessel patency at 90 minutes Circ 1998;97:1549-1556
12 years 5 years p=0.005 p=0.023 Mortality (%) TIMI-0/1 TIMI-2 TIMI-3 Infarct vessel patency at 3-4 weeks Long-term survival after randomisation to Streptokinase: influence of myocardial blood flow JACC 1999;34:62-69
x • Small numbers • No gender matched controls • Post hoc • Sub-analysis • Underpowered etc AHJ 2004;147:133-139
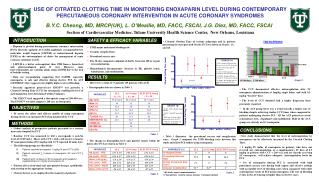
12 - 10 - 8 - 6 - 4 - 2 - 0 No Risk Factors In-Hospital Mortality (%) ≤90 >90-120 >120-150 >150 Door-to-Balloon Time (mins) Effect of Door-to-Balloon Time on Mortality: NRMI 3-4 (n=29,222) JACC 2006;47:2180-2186
12 - 10 - 8 - 6 - 4 - 2 - 0 No Risk Factors ≥1 Risk Factors In-Hospital Mortality (%) ≤90 >90-120 >120-150 >150 Door-to-Balloon Time (mins) Effect of Door-to-Balloon Time on Mortality: NRMI 3-4 (n=29,222) JACC 2006;47:2180-2186
STEMI (NIRMI 3-4)Gender Prelevance (n=29,222) 70.9% Prelevance (n) 29.1% Male Female JACC 2006;47:2180-2186
108 p<0.0001 p<0.0001 6.9% 100 Mortality (%) Door-to-Balloon Time (mins) 3.6% Male Female Male Female STEMI (NIRMI 3-4)Gender Differences (n=29,222) JACC 2006;47:2180-2186
PPCI: Relationship between Door-to-Balloon time and Gender p=0.05 p=0.05 9.9% 7.3% Percentage (%) 6.5% 3.9% >2 hours ≤2 hours Female Female Male Male JAMA 2000;283:2941-2947
Sex-Based Differences in Early Mortality of Patients undergoing Primary Angioplasty for First Acute Myocardial Infarction Circ 2001;104:3034-3038
Prognosis after Myocardial Infarction • Prognosis may be worse in women per se • Women are older at the time of presentation • Women may have more co-morbidity (e.g. shock, hypertension, obesity, renal impairment, diabetes) • Women present later and delay seeking medical attention • Women are under investigated • Women are under treated (less lysis, PCI or CABG)
Physicians recommendations for Cardiac Catheterization: Effects of Race and Gender NEJM 1999;340:618-626
p<0.001 p<0.001 14.5% 32% 9.6% Mortality (%) Revascularisation Rate (%) 20% Male Female Male Female Gender Differences in Revascularisation Rates following AMI AJC 2006;97:1722-1726
p<0.001 p<0.001 60% 54% 52% 45% Patients admitted HREV +ve (%) Revasc Rate in HREV +ve hospitals (%) Male Female Male Female Admission Patterns and Revascularisation Rates following AMI AJC 2006;97:1722-1726
Men Fare Better Women Fare Better All Patients Patients in HREV +ve Patients in HREV –ve Patients REV +ve Patients REV -ve 0 0.5 1.0 1.5 1.75 Odds Ratio [95% CI] Age-adjusted in-hospital mortality with STEMI Men vs. Women AJC 2006;97:1722-1726
Failure of perfusion with thrombolytics alone… RCA occlusion LAD occlusion
Fibrinolysis PCI >90% Availability 100% 50% 0% 10% Availability <50% Treated 5% Reocclusion 54% TIMI 3 0.1% CVA 10% Reocclusion 25% Late Occlusion 1% CVA >90% Treated >90% TIMI 3 Coronary ReperfusionFibrinolysis vs. Percutaneous Intervention Heart 2002;88:298-305
p<0.0001 p=0.0002 p=0.0003 p<0.0001 p=0.0004 Frequency (%) Non-fatal AMI Stroke Death (Non-shock) Combined Death STEMI (PPCI vs. Thrombolysis)Short-term Outcome Gender? Lancet 2003;361:13-20
Death, MI, TVR (30 Day) Bleeding with Abciximab p<0.001 p<0.001 p<0.001 Major Bleed Minor Bleed 12.7% 11.3% Event Rate (%) Patients %) 6.5% 5.8% Female Male Female Male Abciximab Placebo Clinical Benefits of Abciximab is Independent of GenderEPIC, EPILOG, EPISTENT meta-analysis (n=6,595) JACC 2000;36:381-386
STEMI <12 hrs, No shock (N=2,681) Angiographic Criteria fulfilled N=2,082 (73% men, 27% women) Randomise Primary PCI + Abciximab (N=528) Men = 391 Women = 137 Multilink Stent + Abciximab (N=524) Men = 388 Women = 136 Primary PCI (N=518) Men = 370 Women = 148 Multilink Stent (N=512) Men = 371 Women = 141 CADILLAC: Gender based Outcomes Circ 2005;111:1611-1618
CADILLAC: Determinants of One Year Mortality Circ 2005;111:1611-1618
CADILLAC: Baseline Variables Circ 2005;111:1611-1618
CADILLAC: Multivariate Predictors of One Year Mortality in Women Circ 2005;111:1611-1618
Conclusions: AHA Scientific Statement • There is a rising mortality burden in women with CVD • PCI is performed less frequently and with greater delays in women • Better understanding of this disparity should be a priority • RCTs should be developed to specifically assess gender-based, ethnic and racial results of interventional therapy with appropriately matched controls Circ 2005;111:940-953
Conclusions: • Mortality from STEMI is higher in women • Women present later for PPCI • PPCI is performed less frequently in women • Outcomes following PPCI are less favourable in women • Complications of PPCI are higher in women • Present gender specific data are inadequate
X X Time for the Ladies to stop selling themselves short…