Download
1 / 30
491 likes | 1.89k Views
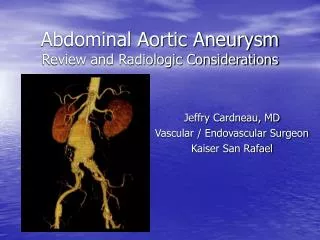
Review on Mycotic Aneurysm. Joint Hospital Surgical Grand Round Li Hoi Man Princess Margaret Hospital 26/4/2014. Content. History Definition Pathogenesis Disease characteristics Diagnosis Treatment. History of Mycotic Aneurysm.

E N D
Review on Mycotic Aneurysm Joint Hospital Surgical Grand Round Li Hoi Man Princess Margaret Hospital 26/4/2014
Content History Definition Pathogenesis Disease characteristics Diagnosis Treatment
History of Mycotic Aneurysm 1844: Rokitansky1 described abscess in the walls of arteries 1851: Koch2 reported the sudden death of a 22/M from a ruptured SMA aneurysm while treating I.E. 1885: Sir William Osler3 proposed a causal relationship between infection of the aortic wall and subsequent aneurysm formation
Definition Initially signified an infected aneurysm found in association with bacterial endocarditis Nowadays denote an infected aneurysm of any type Mycotic aneurysm: both true and false aneurysms that are associated with infection of the arterial wall
Pathogenesis • Oslerian mycotic aneurysms • Embolization of infected cardiac vegetations • Haematogenous seeding • Bacteremia microbial seeding of arteries arteritis aneurysm formation • Infected aneurysms • Bacteremia lodge within the intramural thrombus and arteriosclerotic intima • Others • Mechanical arterial injury with contamination • Contiguous spread
Epidemiology Era of bacterial endocarditis: 2nd -4th decades Now: elderly 6th-8th decades Male predominance (> 2/3) Higher prevalence in drug addicts and patients with AIDS
Clinical presentation • S/S from infection / bacteremia: • S/S secondary to local arterial involvement / aneurysm formation: • Localized tenderness, bruits, neurologic defects, pulsatile masses • Thrombosis / thromboembolization • Rupture • pseudoaneurysm • hypotensive shock, life-threatening haemorrhage
Bacteriology Salmonella choleraesuis, S. typhimurium Staphylococcus aureus Streptococcusspp. Escherichia coli Immunocompromised: Campylobacter spp., Listeria spp., Mycobacterium tuberculosis
Anatomic distribution • Depends on pathology type: • Oslerian: abdominal aorta, femoral artery, SMA • Haematogenous seeding: distal aorta, femoral, iliac and popliteal • Mechanical injury: femoral, brachial
Diagnosis Blood: WCC, ESR Blood cultures: only ~ 60% Arterial Gram stains, cultures, PCR CT and / or MRI Angiography PET-CT
Periaortic fat stranding CTA: irregularity and abrupt truncation of distal SMA arteritis and thromboembolism Fat stranding around SMA arteritis
Gas forming inflammation Hazy aortic wall and gas formation
Periaortic edema and inflammatory soft tissue Hazy aortic wall, para-aortic fluid collection, bilateral pleural effusions, intimal calcification
Prominent periaortic inflammation with destruction of the L3
Diagnosis Blood: WCC, ESR Blood cultures: only ~ 60% Arterial Gram stains, cultures, PCR CT and / or MRI Angiography PET-CT
Diagnosis Blood: WCC, ESR Blood cultures: only ~ 60% Arterial Gram stains, cultures, PCR CT and / or MRI Angiography PET-CT
Principles of Management Control of sepsis Arterial reconstruction
Control of sepsis • Antibiotic therapy • Broad-spectrum, high dose, according to c/st • Extend for at least 6 weeks post-op • Lifelong if prosthetic reconstructions involved • Surgical debridement • Aggressive wide debridement • Drains
Arterial reconstruction Open approach - extra-anatomic reconstruction In-situ reconstruction-EVAR
Conventional open surgery Debridement of infected tissues Stump closure
Extra-anatomic reconstruction • Conventional approach • Lower reoperation rate for graft infection • High mortality rate 20,21(23-39%) • Complications: • aortic stump blowout • extra-anatomic bypass occlusion • recurrent aortoenteric fistula • recurrent graft infection9 (up to 13%)
In-situ reconstruction: EVAR • EVAR • Rapid control of haemorrhage • Reduced surgical morbidity and mortality • Places a graft in direct proximity to the infection • Does not afford the opportunity to debride infected tissue • In combination with prolonged antibiotics and use of drainage offer resolution of arterial infection
Comparison between open vs EVAR Kan12 reviewed on efficacy of EVAR in infected AAA, 41cases, EVAR (n=20) vs conventional surgery (n=21) • Early (30 days) post-op mortality similar • Late (2 year) mortality greater in conventional surgery (10% vs 25%) • Aneurysm-related event-free survival similar
References: Rokitansky: Handbuch der pathologischen Anatomie, Ed 2, 1844, p55 Koch: Uber Aneurysma der Arteriae mesenterichae superioris, 1851, Erlangen Osler: The Buslstonian lectures on malignant endocarditis Crane: Primary multilocular mycotic aneurysm of the aorta. Arch Patho 24: 634, 1937 Ponfick: Uber embolische Aneurysmen, nebst Bemerkungen uber das acute Herzaneurysma. Virchows Arch 58: 528, 1873 Eppinger: Pathogenese der Aneurysmen einschliesslich des Aneurysma equiverminosum. Arch Klin Chir 35: 404, 1887 Revell: Primary mycotic aneurysms. Ann Intern Med 22:431, 1943 Hawkins: Primary mycotic aneurysms. Surgery 40:747, 1956 Ewart: Spontaneous abdominal aortic infections: essentials of diagnosis and management. Am Surg 49: 37, 1983 Berchtold: Endovascular treatment and complete regression of an infected AAA. J Endovasc Ther 9: 543, 2002 Koeppel: mycotic aneurysm of the abdominal aorta with retroperitoneal abscess: successful endosvascular repair. J Vasc Surg 40: 164, 2004 Kan: The efficacy of aortic stent grafts in the management of mycotic abdominal aortic aneurysm institute case management with systemic literature comparison. Ann Vasc Surg 24(4): 433-440, 2010 Forbes: Endovascular repair of Salmonella-infected AAAs: a word of caution. J Vasc Surg 44(1): 198-200, 2006 Vallejo: The changing management of primary mycotic aortic aneurysms. J Vasc Surg 2011 Lee: In situ versus extra-anatomic reconstruction for primary infected infrarenal AAA. J vasc Surg 54(1): 64-70,2011 Brown: Arterial reconstruction with cryopreserved human allografts in the setting of infection: a single-center experience with midterm FU. J Vasc Surg 49(3): 660-666, 2009 Gelabert: Primary Arterial infections and antibiotic prophylasix. Vascular and Endovascular Surgery – a comprehesive review 157-177 Perler: Infected aneurysm. Vascular Surgery Principles and Practice Ed3 669-686 Semba: Mycotic aneurysms of the thoracic aorta: repair with use of endovascular stent grafts. J Vasc Interv Radiol 1998; 9: 33-40 Leon: Diagnosis and Management of aortic mycotic aneurysms. Vasc and Endova Surg 44(1) 5-13, 2010 Stone: Comparison of open and endovascular repair of inflammatory aortic aneurysms. J Vasc Surg 10-2012 951-6
Our cases M/65, GPH, walks unaided LLQ pain with radiation to back and subjective fever for 1/52 Temp 37.7 abd: 5cm expansile mass, tender CT: 5.2cm infra-renal AAA with impending rupture and para-aortic fat stranding Put on augmentin and flagyl Blood c/st, TB, widal test, Treponema: all –ve EVAR done FU CT showed no endoleak and aortic sac wall thickening showed interval improvement Lifelong levofloxacin 750mg daily
Our cases M/65 GPH Abd pain x 1/12 CT: 2.9cm infrarenal AAA with eccentric mural thrombus EVAR + fem-fem bypass on 5/2010 Blood C/st: salmonella sensitive to ciprofloxacin Subsequent CT: resolution of the inflammatory changes Antibiotic coverage discontinued 1 year later FU CT 2.5 years later: ? Relapse of infection with increased perigraft soft tissue swelling Treated with a 8-week course of rocephin 2gm daily then changed to azithromycin 500mg daily po afterwards