Download
1 / 53
930 likes | 2.52k Views
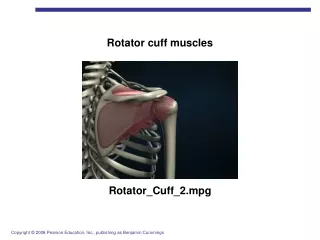
MR Imaging of the Rotator Cuff. Timothy G. Sanders, M.D. MRI Technique. -T1 and T2 FS -Oblique Coronal. -T1 and T2 FS -Oblique Sagittal. -T2 FS and GRE -Axial. Osseous Outlet and Acromion. Rotator Cuff Surrounded by a Bony Arch Mechanical Impingement leads to degeneration of the cuff

E N D
MR Imaging of the Rotator Cuff Timothy G. Sanders, M.D.
MRI Technique -T1 and T2 FS -Oblique Coronal -T1 and T2 FS -Oblique Sagittal -T2 FS and GRE -Axial
Osseous Outlet and Acromion • Rotator Cuff Surrounded by a Bony Arch • Mechanical Impingement leads to degeneration of the cuff • Anterior Acromion Most Important Structure Leading to Impingement
Normal Osseous Outlet Clavicle Acromion Coracoid
Acromial Types Type I
Acromial Types Type II
Acromial Types Type III
Acromial Types Type IV
Acromial Down Sloping Anterior Down Sloping Evaluated on Sagittal Images Axis of Acromion Normal Axis of Acromion Anterior Down Sloping
Acromial Down Sloping Lateral Down Sloping Evaluated on Coronal Images Axis of Acromion Normal Axis of Acromion Lateral Down Sloping
Acromial Spur -Spur -Contains Marrow Signal -Deltoid Tendon (Mimics Spur) -Black (No Marrow Signal)
Os Acromiale Ossification Center Usually Closes by 22-25 y.o. Normal Appearing Anterior Acromion on Axial Image
Os Acromiale (Axial Images) -Can be unstable resulting in impingement of Rotator Cuff during contraction of the deltoid
Os Acromiale (Sagittal Images) Normal AC Joint “Double” AC Joint Sign
Os Acromiale AC Joint Os Acromiale “Double” AC Joint
Acromion • Type (I, II, III) • Anterior/ Lateral Down Sloping • Inferior Spur • Os Acromiale
Coracoacromial Ligament -Thick Ligament can Impinge on Anterior Rotator Cuff -Normal Ligament <3 mm
Acromioclavicular Joint -Does it cause mass effect on rotator cuff? -AC degenerative change, capsular hypertrophy -Cuff less rigidly confined
AC Joint Sprain/Separation Grade I -Capsular edema, effusion -No elevation Grade II -Capsular edema, effusion -Elevation distal clavicle
Osteolysis of Distal Clavicle Post-traumatic osteolysis -Complication of trauma (occurs within 2 months of injury, self limiting) -Repetitive stress (wt. lifters) -X-ray: loss of normal cortical line- distal clavicle
Coracoid Impingement -Narrowed C-H Distance can Impinge on Subscapularis -Normal Coracohumeral Distance is 11 mm
Osseous Outlet and Acromion • Acromion • Type, Down Sloping, Spur, Os Acromiale • AC Joint • Deg. Change, Hypertrophy (mass effect?) • Coracoacromial Ligament (thickened?) • Coracohumeral Impingement (subscap?)
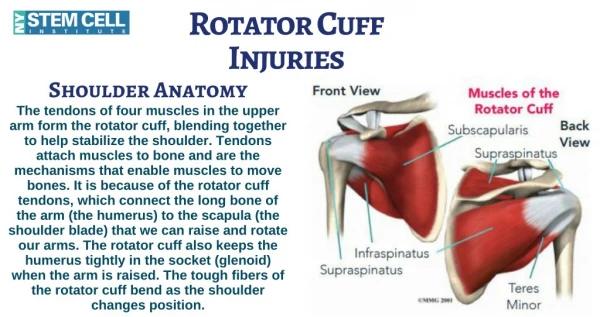
Rotator Cuff (Sagittal) Supraspinatus; Infraspinatus; Teres Minor; Subscapularis
Rotator Cuff (Coronal) -Primary Plane for Evaluating the Supraspinatus Tendon -Musculotendinous Junction at 12:00 Position
Rotator Cuff (Axial Plane) -Supraspinatus Tendon
Rotator Cuff (Axial Plane) -Primary Plane for Evaluating Subscapularis -Infraspinatus Located Posteriorly
Rotator Cuff (Coronal) -Subscapularis - Located Anteriorly - Multi-slip tendon - Infraspinatus - Located Posteriorly - Slopes upward
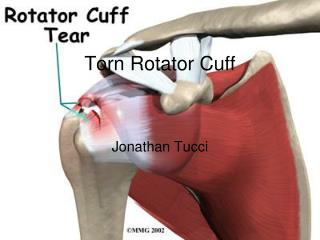
Rotator Cuff Pathology • Tendonopathy • Tear • Partial Thickness, Full Thickness, Complete • Musculotendinous Retraction • Fatty Atrophy • HADD/ Calcific Tendonitis
Tendonopathy -Increased T1-signal; thickened/ attritional changes (thinned) -Intermediate T2-signal (No Fluid Signal)
Partial Thickness Tear (Articular) -T2: Fluid Signal extending into black tendon -Partial Thickness Undersurface Tear
Partial Thickness Tear (Bursal) -Fluid Signal Extending into the Bursal Surface of the Supraspinatus Tendon
Partial Thickness Tear (Interstitial) -Fluid Signal within the Substance of the Tendon -Does Not Involve the Articular or Bursal Surface
Intramuscular Cyst Rotator Cuff -High Association with 1. P.T. Undersurface Tear 2. Small F.T. Tear 3. DDX: Paralabral Cyst
Intramuscular Cyst Rotator Cuff -Intramuscular Cyst Supraspinatus -Small Undersurface P.T. Tear
Full Thickness Tear -Fluid extends through the entire thickness of the tendon (superior to inferior) -Mild retraction of musculotendinous junction
Massive Tear Musculotendinous retraction -Measure in centimeters; can affect prognosis
Fatty Atrophy -Mild, Moderate, Severe -Streaks of high signal on T1 -Loss of muscle bulk (Sagittal)
Calcific Tendonitis -HADD: Dark Globular Area on all Pulse Sequences -Blooming Artifact on Gradient Echo Images
Subscapularis -Subscapularis: Attaches to lesser tuberosity -Extra-articular Biceps: Best Seen on Axial Image -In Bicipital Groove; Transverse Ligament
Avulsion of Subscapularis -Subscapularis Muscle can Avulse off of Lesser Tuberosity -Associated with Dislocation of the Biceps Tendon -Seen best in Axial Plane
CH Ligament Biceps Tendon (Anatomy) LHBT LHBT • Coracohumeral ligament primary stabilizer of LHBT
Biceps Tendonitis/ Tear -Thick Tendon; Increased Signal -Intra-articular -Extra-articular
Biceps Tendon (Anatomy) • Subscapularis/ transverse humeral ligament • Secondary stabilizer
Biceps Subluxation: Pattern I • CHL: intact • 2. Subscapularis tendon: complete tear • - No Dislocation of LHBT
Pattern II: Intra-articular • CHL: torn • Subscapularis tendon: complete tear • - Intra-articular dislocation of LHBT