Download
1 / 15
150 likes | 167 Views
Explore the anatomy of venous blood sinuses in the brain, their functions, and connections with various veins to better understand cerebrovascular physiology.

E N D
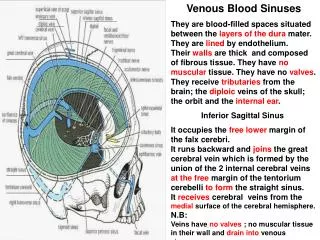
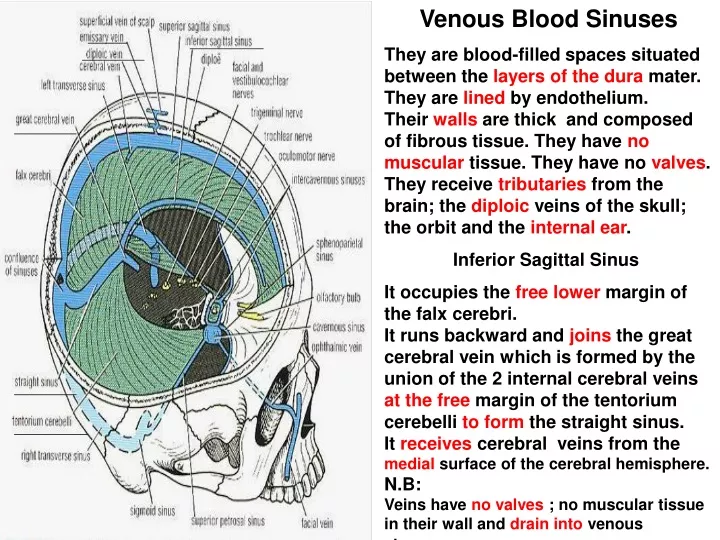
Venous Blood Sinuses They are blood-filled spaces situated between the layers of the dura mater. They are lined by endothelium. Their walls are thick and composed of fibrous tissue. They have no muscular tissue. They have no valves. They receive tributaries from the brain; the diploic veins of the skull; the orbit and the internal ear. Inferior Sagittal Sinus It occupies the free lower margin of the falx cerebri. It runs backward and joins the great cerebral vein which is formed by the union of the 2 internal cerebral veins at the free margin of the tentorium cerebelli to form the straight sinus. It receives cerebral veins from themedial surface of the cerebral hemisphere. N.B: Veins have no valves ; no muscular tissue in their wall and drain into venous sinuses
Superior Sagittal Sinus It occupies the upper fixed border of the falx cerebri. It begins in the front at the foramencecum where it receives a vein from the nasal cavity. It runs backward, grooving the vault of the skull and at the internal occipitalprotuberance it deviates to one side ( usually the right ) and becomes continuous with the transverse sinus. It communicates through small openings with 2 or 3 venous lacunae on each side. Numerous arachnoid villi and granulations project into these lacunae which also receive the diploic; emissary and meningeal veins. It receives the superior cerebral veins . At the internal occipital protuberance it is dilated to form the confluence of the sinuses which is connected to the opposite transverse sinus and receives the occipital sinus.
Straight Sinus It occupies the line of junction of the falx cerebri with the tentorium cerebelli. It is formed by the union of the inferior sagittal sinus with the great cerebral vein. It ends by turning to the left ( sometimes to the right ) to form the transverse sinus.
Occipital Sinus It is a small sinus occupying the attached margin of the falx cerebelli. It communicates with the vertebral veins near the foramen magnum. Superiorly it drains into the confluence of sinuses.
Transverse Sinus They are paired and begin at the internal occipital protuberance. The right sinus usually continuous with the superior sagittal sinus. The left is continuous with the straight sinus. Each sinus occupies the attached margin of the tentorium cerebelli , grooving the occipital bone and posteroinferior angle of the parietal bone. They receive the superior petrosal sinuses; inferior cerebral and cerebellar veins and diploic veins. They end by turning downward as the sigmoid sinuses.
Superior and Inferior Petrosal Sinuses They are small and situated on the superior and inferior borders of the petrous part of the temporal bone on each side. Each superior sinus drains the cavernous sinus into the transverse sinus. Each inferior sinus drains the cavernous sinus into the internal jugular vein.
Sigmoid Sinuses They are a direct continuation of the transverse sinuses. Each sinus turns downward and medially and grooves the mastoid part of the temporal bone. Here it lies behind the mastoid antrum. It then turns downward through the posterior part of the jugular foramen to become continuous with the superior bulb of the internal jugular vein.
Cavernous Sinuses They are situatedin the middle cranial fossa on each side of the body of the sphenoid bone. Each sinus extends from the superior orbital fissure in front to the apex of the petrous part of the temporal bone behind. The 3rd ; 4th cranial nerves and the ophthalmic & maxillary divisions of the trigeminal nerve run forward in the lateral wall of this sinus. They lie between the endothelial and the dura mater . The internal carotid artery, its sympathetic nerve plexus and abducent nerve run forward through it. They are separated from the blood by an endothelial covering.
5 1 5 The tributaries are 1- Superior ophthalmic vein which communicates it with thefacial V 2- Inferior ophthalmic vein. 3- Cerebral veins 4- Central vein of the retina 5- Sphenopareital sinus.The sinus drains posteriorly into the superior and inferior petrosal sinuses and inferiorly into the pterygoid venous plexus. The 2 sinuses communicate with one another by means of the anterior and posterior intercavernous sinuses which run in the diaphragma sellae in front and behind the stalk of the hypophysis cerebri.
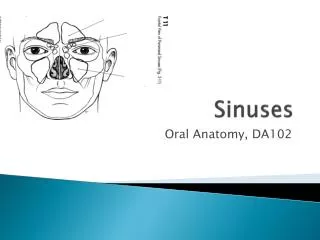
Hypophysis Cerebri The pituitary gland is an edocrine gland. It is small, oval and attached to the undersurface of the brain by infundibulum. It is located in the sella turcica of the sphenoid bone. It is divided into an anterior lobe or adenohypophysis and posterior lobe or neurohypophysis. Relations Superiorly: The diaphragma sellae which has a central aperture that allows the passage of the infundibulum. This sellae separates the anterior lobe from the optic chiasma. Inferiorly: The body of the sphenoid with its sphenoid air sinuses. Laterally: The cavernous sinus and its contents. Posteriorly: The dorsum sellae; basilar artery and pons. Blood supply: The superior and inferiorhypophyseal arteries the branches of the internal carotid artery. Veins drain into the intercavernous sinuses.
Clinical Notes Hypophyseal enlargement and Optic chiasma A pituitary tumor pushes the diaphragma sellae upward and causes pressure on the optic chiasma. This results in interference with the function of the nerve fibers crossing in the chiasma ( from the inner quadrants of the retina ) and the patient presents with bitemporal hemianopia. Further expansion of the pituitary tumor causes erosion of the body of the sphenoid bone.
Extradural Hemorrhage It results from injuries of the meningealarteries or veins. The most common is the anterior branch of the middle meningeal artery. A minor blow to the side of the head result in fracture of the anteroinferior portion of the parietal bone ( pterion ). The intracranial pressure rises. The blood clot exerts local pressure on the underlying motor area in the precentral gyrus. Blood may pass out through the fracture line to form a soft swelling under the temporalis muscle. The burr hole through the skull wall should be placed 2.5 to 4 cm above the midpoint of the zygomatic arch to ligate or plug the torn artery or vein.
Subdural Hemorrhage It is more common than the middle meningeal artery hemorrhage. It results from tearing of the superior cerebral veins at their entrance into the superior sagittal sinus. The cause is a blow on the front or back of the head causing anteroposterior displacement of the brain within the skull. Blood under low pressure begins to accumulate in the space between the dura and arachnoid. The case is bilateral in 50 %. Acute symptoms in the form of vomiting due to rise in the venous pressure may be present. In the chronic form, over a several months, the small blood clot will attract fluid by osmosis so a hemorrhagic cyst is formed and gradually expands produces pressure symptoms.
Intracranial Hemorrhage in the Infant It occurs during birth and from excessive molding of the head. Bleeding occurs from cerebral veins or venous sinuses Excessive anteroposterior compression often tears the anterior attachment of the falx cerebri from the tentorium cerebelli. bleeding then takes place from the great cerebral veins; straight sinus or inferiorsagittal sinus.
Subarachnoid Hemorrahage It results from leakage or rupture of a congenital aneurysm on the circle of Willis or less commonly from an angioma. The sudden symptoms include severe headache; stiffness of the neck and loss of consciousness. The diagnosis is established by withdrawing heavily blood- stained CSF fluid through a lumbar puncture ( spinal tap ). Cerebral Hemorrhage It is caused rupture of the thin-walled lenticulostriate artery, a branch of the middle cerebral artery. The hemorrhage involves the vital corticobulbar & corticospinal fibers in the internal capsule and produces hemiplegia on the opposite side of the body. The patient immediately loses consciouness and paralysis is evident when consciousness regained.