Download
1 / 18
180 likes | 326 Views
Clostridium-Difficile Reduction Utilizing an Interdepartmental Team Approach Mary Jane Lamb RN, IP. Objectives. Demonstrate how APIE was used to facilitate solving our problem Discuss how our team approach helped to improve care, reduce C-Diff #s and make staff happier

E N D
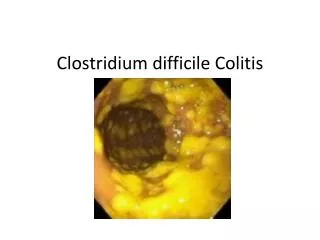
Clostridium-Difficile Reduction Utilizing an Interdepartmental Team Approach Mary Jane Lamb RN, IP
Objectives • Demonstrate how APIE was used to facilitate solving our problem • Discuss how our team approach helped to improve care, reduce C-Diff #s and make staff happier • Discuss most recent changes to isolation and to lab testing
APIE • Assess • Plan • Initiate • Evaluate
Assess Problem Identify problem Increase in cases - 14 cases in 2007
Assess Problem Identify problem Increase in cases - 14 cases in 2007 18 CASES IN 2008 FROM JANUARY TO JUNE
Assess Problem Identify problem Increase in cases- 14 cases in 2007 18 cases in 2008 Jan – June Time Line • Indentify overlapping patients • Indentify primary departments involved Observe staff behavior • Not isolating until after diagnosis • Sharing commodes/toilets • Carrying dirty laundry out of room to hamper
Plan • Target Zero Task Force – Interdepartmental RNs, CNAs, Education staff, and Environmental staff 2. Review Policy and Procedure 3. Meetings with Patient Care Staff, Environmental Staff and Education
Implement 1. Revise Isolation Policies and C-Difficile Policy • All patients with diarrhea on isolation until cleared • Strict Contact Isolation • Double bag linen and trash 2. Mandatory education classes for all patient care staff 3. Revise Terminal Cleaning Policy • Expanded terminal cleaning • Wall to floor • Privacy curtains 4. Environmental Service education
Implement • 5. Add 2 Environmental FTEs for full 24/7 coverage
Evaluate 1. Staff reactions and concerns • Anger over number of isolation rooms • Concern over increase in isolation PPE • Concern/anger over extra time involved • Concern by Environmental staff that Patient Care staff was not using proper technique • Revise Isolation Policy again • Listened to concerns of Patient Care staff and Environmental staff
Evaluate • Decrease in C-Difficile numbers!!!!!
Immediate decrease in C-Difficile numbers 2007 – 14 cases/21796 X 10000 = Rate 6.0 2008 - 22 cases/21631 X 10000 = Rate 10.0 18 cases in 1st 6 months 4 cases in 2nd 6 months 2009 - 11 cases/20674 X 10000 = Rate 5.0 2010 - 8 cases/20255 X 10000 = Rate 4.0 2011 - 4 cases/14523 X 10000 = Rate 2.7 through Sept.
2011 Changes • New Policy and Procedure Including definition of diarrhea • 3 loose stools in 24 hours Reemphasize when testing can be done • only 1 per day Decrease in Isolation time • stop isolation 24 hours after diarrhea stops Developed algorithm for C-Dif isolation
Patient has loose stool Initiate Contact Plus Isolation 3 or > loose stool In 24 hours No diarrhea or < 3 bouts in 24hs Obtain MD order for C-Diff test • Discontinue isolation • d/c stool testing with MD order C-Diff positive All cultures negative Continue isolation Note: If MD has ordered C-diff test and pt. has formed stool assess need for test with MD. Pt does not need isolation. Loose stools cease X 24 hrs Terminally Clean room D/C Isolation
NEW ISOLATION CATEGORY Contact Plus – used for C-Difficile and other organisms that are not effected by alcohol hand gel/foam • Gloves and gowns when entering room to touch anything in environment • Hand washing with soap and water
Toxigenic C- Difficile Testing NAAT – nucleic acid amplification method • This assay utilizes DNA amplification to detect the pathogenicity locus (Paloc) • Sensitivity and Specificity rates>95% • Neg predictive value of 99% • Pos predictive value of 92%
Testing Criteria Significant Diarrhea – 3 or more per 24 hours Submit Only 1 unformed stool • watery, loose, or taking the form of container Only 1 specimen will be accepted per diarrheal episode • Due to high sensitivity of negative test-no need to repeat • “Test for cure” for positive test not appropriate because patient may carry toxigenic C-Difficile for months after clinical cure Rare form stools may be accepted with approval of Lab Medical Director when requested by physician.