Download
1 / 41
420 likes | 606 Views
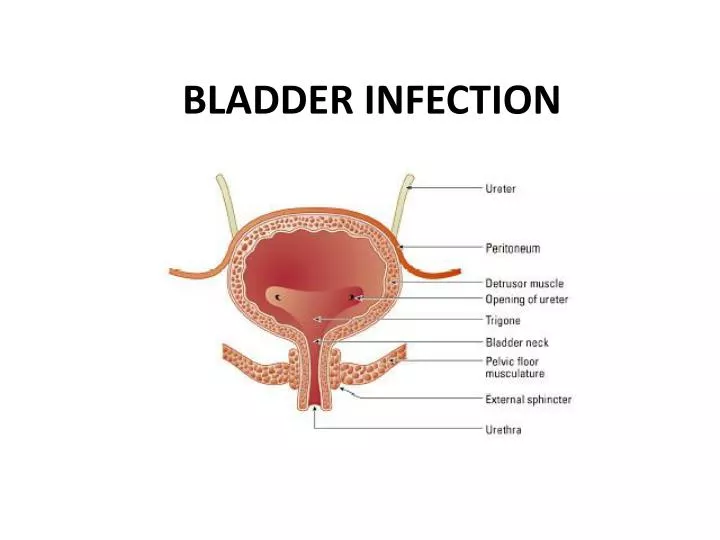
BLADDER INFECTION. Acute Cystitis. Definition: refers to urinary infection of the lower urinary tract, particularly the bladder. Sex Predilection: F>M 1 ° Mode of infection: ascending from the periurethral /vaginal and fecal flora D iagnosis is made clinically.

E N D
Acute Cystitis • Definition: refers to urinary infection of the lower urinary tract, particularly the bladder. • Sex Predilection: F>M • 1° Mode of infection: ascending from the periurethral/vaginal and fecal flora • Diagnosis is made clinically
Acute Cystits: Presentation and Findings • Frequent Findings: Irritative voiding symptoms (dysuria, frequency, urgency) • Other common symptoms: low back and suprapubic pain, hematuria, cloudy/foul-smelling urine • Fever and systemic symptoms: rare • Urinalysis: (+) WBC, (+) Hematuria • Urine Culture: confirm the diagnosis • E. coli – most common • Others: G(-) Klebsiella and Proteus; G(+) S. saprophyticus and Enterococcus.
Management Pharmacologic • Short course oral antibiotics • Trimethoprim-sulfamethoxazole, Nitrofurantoin, and Fluoroquinolones • Duration: 3-5 days • fluoroquinolones with long half-lives (fleroxacin, pefloxacin, and rufloxacin) may be suitable for single-dose therapy
Recurrent Cystitis/UTI • Presentation and Findings: • Cause: bacterial persistence or reinfection with another organism • Note: it’s important to identify the cause • Bacterial Persistence – remove the infected source • Reinfection – Preventive therapy
Bacterial Persistence Radiologic imaging is indicated US – provide a screening evaluation of the GUT IVP, Cystoscopy, CT may sometimes be necessary Frequent, recurrent UTI – bacterial localization studies Bacterial Reinfection Evaluate for evidence of vesicovaginal or vesicoenteric fistula Otherwise, radiologic examination is not necessary Radiographic Imaging
Management • Depends on the cause: • Surgical removal of the infected source, i.e. urinary calculi – treat persistence • Reinfection: Surgical repair of fistulas, prophylactic antibiotics • Recurrent UTI/cystitis related to sexual activity: • Frequent emptying of the bladder and a single dose of antibiotic taken after intercourse • Alternative Tx for recurrent cystits/UTI • Intravaginal estriol, lactobacillus vaginal suppositories, cranberry juice
Malacoplakia • Uncommon inflammatory disease of the bladder • manifesting as plaques or nodules made up of large histiocytes (von Hansenmann cells) and laminar inclusion bodies (Michaelis-Gutmann bodies) • Can also affect ureters, kidneys
Presentation and Findings • Patients • F>M with history of UTI • With chronic illness or immunosuppressed • Signs and Symptoms • Bladder: Irritative voiding symptoms – urgency and frequency; and hematuria • Ureter and Kidney: fever, flank pain, flank mass • Both kidneys: s/sx of azotemia and renal failure
Radiologic Findings • US/CT • May demonstrate a mass in the bladder and and evidence of obstruction. • KIDNEY: focal, diffuse, hypodense parenchymal masses on CT • Biopsy • Differentiates malakoplakia from malignancy
Management Pharmacologic • Primarily consists of antibiotic therapy with high intracellular levels: • TMP-SMX and fluoroquinolones • Bethanecol and Ascorbic Acid – enhance phagolysosomal activity • Lower urinary tract involvement: • Antibiotic alone Non-pharmacologic • Involvement of ureter or kidney: • surgical excision • Prognosis is poor and mortality is high in patients who have bilateral renal involvement regardless of treatment
ANATOMY Chestnut-shaped fibromuscular and glandular organ Inferior to bladder 20g; 3cm diameter produces prostate fluid
PROSTATE INFECTIONS I. Acute Bacterial Prostatitis II. Chronic Bacterial Prostatitis III. GranulomatousProstatitis IV. Prostate Abscess
I. Acute Bacterial Prostatis • Inflammation of the prostate associated w/ a UTI • From urethral infection or reflux of infected urine • Luekocytes are seen within the surrounding acini of the prostate in response to infection • Edema and hyperemia developed • Prolong infection – necrosis and abscess
Presentation and Findings • More common in adults esp. <50 (Collins et al, 1998) • abrupt onset • fever, chills, malaise, arthralgia, myalgia, lower back/rectal/perineal pain • urinary symptoms (frequency,urgency, dysuria) • Urinary retention • DRE - tender, enlarged glands that are irregular and warm
ACUTE BACTERIAL PROSTITIS LABS • Urinalysis -WBCs and occasionally hematuria • Serum Blood Analysis– leukocytosis • Prostate-specific antigen DEFINITIVE DX • microscopic examination and culture of the prostatic expressate • culture of urine obtained before and after prostate massage – single organism • E. coli – most causative agent • OTHERS: Proteus, Klebsiella, Enterobacter,Pseudomonas, and Serratia spp.
ACUTE BACTERIAL PROSTITIS RADIOLOGIC IMAGING • Rarely indicated • Bladder ultrasonography – useful in determining the amount of residual urine MANAGEMENT • Pharmacologic • Trimethoprim and Fluoroquinolones (4–6 weeks) • Ampicillin and an aminoglycoside for gram-negative bacteria and enterococci • Non-pharmacologic • Patients w/ urinary retention 2nd to acute prostatis - suprapubiccatheter
II. Chronic Bacterial Prostatis CLINICAL PRESENTATION • more insidious onset • characterized by relapsing, recurrent UTI caused by the persistence of pathogen in the prostatic fluid despite antibiotic therapy • dysuria, urgency, frequency, nocturia, and low back/perinealpain • DRE: often normal; occasionally, tenderness, firmness, or prostatic calculi
Chronic Bacterial Prostatis LABS • Urinalysis - a variable degree of WBCs and bacteria • Serum Blood Analysis– no leukocytosis • Prostate-specific antigen DEFINITIVE DX • microscopic examination and culture of the prostatic expressate using the 4-cup test • E. coli – most causative agent
The 4-cup Test • Preparation: • Require Px to have a full bladder • Retract foreskin of uncircumcised men • Clean glans with soap/water or povidone-iodine • Collection: • -Collect first 10ml of voided urine (VB1) • -Discard next 100ml • -Collect next 10ml of voided urine (VB2) • -Massage prostate and collect prostate expressate (EPS) • -Collect first 10ml of voided urine after massage (VB3) • -Immediately culture and microscopically examine all specimens • Interpretation: • -All specimens <103 CFU/ml = not bacterial prostatitis • -VB3 or EPS >10 x CFU of VB1 = chronic bacterial prostatitis • -VB1 > other specimens = urethritis or specimen contamination • -All specimens >103 CFU/ml = treat for UTI and repeat test
ACUTE BACTERIAL PROSTITIS RADIOLOGIC IMAGING • Rarely indicated • Transrectalultrasonography – if prostatic abscess MANAGEMENT • Pharmacologic • Antibiotic similar to acute bacterial prostatis but for 3-4 months • TMP-SMX 1 single-strength tablet daily, nitrofurantoin 100 mg daily, or ciprofloxacin 250 mg daily • Non-pharmacologic • Transurethral resection of the prostate - refractory disease
III. GranulomatousProstatis Etiology: • bacterial, viral, or fungal infection, • the use of bacillus Calmette-Guerin therapy • malacoplakia, or systemic granulomatous diseases affecting the prostate • 2/3 of cases have no specific cause 2 types of Non-specific granulomatousprostatitis: • Non-eosinophilic – abnormal tissue response to extravasated prostatic fluid • Eosinophilic – more severe, allergic response of prostate to some unknown antigen
GranulomatousProstatis CLINICAL PRESENTATION • fever, chills, and obstructive/irritative voiding symptoms • urinary retention • eosinophilicgranulomatousprostatitis - severely ill and have high fevers • DRE - hard, indurated, and fixed prostate, difficult to distinguish from prostate carcinoma
GranulomatousProstatis LABS • Urinalysis – no evidence of bacterial infection • CBC – leukocytosis; marked eosinophilia DEFINITIVE DX: biopsy of prostate MANAGEMENT • Pharmacologic • Antibiotic therapy and corticosteroids • Non-pharmacologic • Transurethral resection of the prostate - patients who do not respond to treatment and have significant outlet obstruction.
IV. Prostate Abscess • result from complications of acute bacterial prostatitis • High risk: • Diabetes • those receiving chronic dialysis • immunocompromised patients, undergoing urethral instrumentation, who have chronic indwelling catheters • Clinical Presentation • Similar Symptoms as acute bacterial prostatitis • History of acute bacterial prostatitis with good initial response to antibiotics but recurrence of symptoms during Tratment • DRE: tender and swollen prostate; fluctuance 16% px
Prostate Abscess RADIOLOGIC IMAGING • transrectalultrasonography or pelvic CT scan is crucial for diagnosis and treatment MANAGEMENT • Pharmacologic • Antibiotic therapy • Non-pharmacologic • Transrectal drainage • Transurethral resection and drainage
Urethritis • Infection / inflammation of the urethra • Categorized into: • Neisseriagonorrhea • Other organisms • Chlamydia trachomatis, Ureaplasmaurealyticum, Trichomonasvaginalis, and Herpes Simplex Virus • Acquired through sexual intercourse
URETHRITIS PRESENTATION AND FINDINGS • urethral discharge and dysuria • Obstructive voiding symptoms - patients with recurrent infection • 40% of patients with gonococcalurethritis are asymptomatic DIAGNOSIS • examination and culture of the urethra
URETHRITIS RADIOLOGIC IMAGING • Retrograde urethrogram - indicated in patients with recurrent infection and obstructive voiding symptoms MANAGEMENT • Pharmacologic • Gonococcal: ceftriaxone (250 mg intramuscularly); fluoroquinolones (ciprofloxacin 250 mg or norfloxacin 800mg) • Non-gonococcal: tetracycline or erythromycin (500 mg 4 times daily) or doxycycline (100 mg twice daily) for 7–14 days • Non-pharmacologic • Prevention! • Protective sexual practices
URETHRITIS Female: urethral discharge Male: urethral discharge
Epididymitis • Infection / inflammation of the epididymis • ascending infection of the lower urinary tract • Men <35 y/o STDs (N. gonorrhoeaeand C. trachomatis) • Children & older men urinary patogens (E. coli) • Homosexual men E. coli • may spread to involve the testis
Epididymitis • Presentation & Findings • Severe scrotal pain that may radiate to the groin or flank • Scrotal enlargement or reactive hydrocele • Urethritis, cystitis or prostatitis • PE: • enlarged and red scrotum • Thickened spermatic cord
Epididymitis • Presentation and Findings • Urinalysis: WBCs and bacteria in the urine or urethral discharge • Serum blood analysis: leukocytosis • Radiologic Imaging • Scrotal Doppler UTZ or radionuclide scanning • Epididymitis: enlarged epididymis with increased blood flow
Epididymitis Management • Pharmacologic • Oral Antibiotics and NSAIDS • Treatment of sexual partners in STD • Non-pharmacologic • Bed rest, scrotal elevation & NSAIDS – helpful in reducing the duration of symptoms • Sepsis or severe infection hospitalization & parenteral antibiotic therapy • Abscess open drainage • Chronic, relapsing epididymitis & scrotal pain epididymectomy
EPIDIDYMITIS & URETHRITIS IN HIV PATIENTS • caused by N. gonorrhoeae and C. trachomatis • E. coli is more common • HIV-infected patients with suppurative or antibiotic-resistant epididymitis - infection with fungi or mycobacteria should be considered • it is recommended that HIV-infected patients abstain from sexual intercourse until 7 days after treatment is completed.
REFERENCE: • Smith’s General Urology 17th Edition • Images from http://images.google.com.ph