Download
1 / 14
270 likes | 835 Views
Fate of Macrophages in inflammation. After the initiating stimulus is eliminated and the inflammatory reaction abates, macrophages eventually die or wander off into lymphatics . In chronic inflammatory sites, however, macrophage accumulation persists by: 1- macrophages can proliferate .

E N D
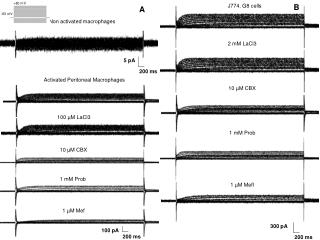
Fate of Macrophages in inflammation • After the initiating stimulus is eliminated and the inflammatory reaction abates, macrophages eventually die or wander off into lymphatics. • In chronic inflammatory sites, however, macrophage accumulation persists by: 1- macrophages can proliferate. 2- Steady release of lymphocyte-derived chemokines and other cytokines get the macrophges immobilized in inflammatory sites. • IFN-γ can also induce macrophages to fuse into large, multinucleated cells called giant cells
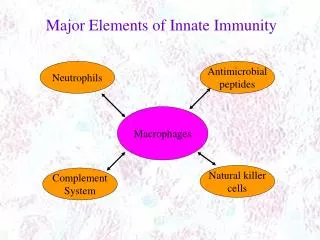
Lymphocytes, Plasma Cells, Eosinophils, and Mast Cells • Lymphocytes and macrophages interact in a bidirectional way, and these interactions play an important role in chronic inflammation • Activated T lymphocytesproduce cytokines, including IFN-γ, a powerful activator of macrophages, promoting more antigen presentation and cytokine secretion • Plasmacells develop from activated B lymphocytes and produce antibodies directed either against persistent antigens in the inflammatory site or against altered tissue components
Eosinophils • are characteristically found in inflammatory sites around parasitic infections or as part of immune reactions mediated by IgE, typically associated with allergies. • Their recruitment is driven by adhesion molecules similar to those used by neutrophils, and by specific chemokines (e.g., eotaxin) derived from leukocytes or epithelial cells. • Eosinophil granules contain major basic protein, a highly charged cationic protein that is toxic to parasites but also causes epithelial cell necrosis
Mast cells • are sentinel cells widely distributed in connective tissues throughout the body • can participate in both acute and chronic inflammatory responses. • IgE-armed mast cells are central players in allergic reactions, including anaphylactic shock. • Mast cells can also elaborate cytokines such as TNF and chemokines • In individuals with atopy(individuals prone to allergic reactions), mast cells are "armed" with IgE antibody specific for certain environmental antigens. When these antigens are subsequently encountered, the IgE-coated mast cells are triggered to release histamines and AA metabolites that elicit the early vascular changes of acute inflammation.
GranulomatousInflammtion -Aggregates of epithelioidhistiocytes -Mechanism: • Persistent T-cell response to certain microbes as M. tuberculosis, • Foreign bodies. E.g. suture, splinter. • Diseases associated with granulomatous inflammation: • Tuberculosis • Leprosy
Granuloma morphology • Macrophages in granulomas have pink, granular cytoplasm with indistinct cell boundaries. The aggregates of epithelioid macrophages are surrounded by a collar of lymphocytes secreting the cytokines responsible for continuing macrophage activation. • Older granulomas may have a rim of fibroblasts and connective tissue, and frequently, multinucleated giant cells
a combination of hypoxia and free-radical injury leads to a central zone of necrosis. Grossly, this has a granular, cheesy appearance and is therefore called caseousnecrosis. Microscopically, this necrotic material appears as amorphous, structureless, granular debris, with complete loss of cellular details. • Healing of granulomas is accompanied by fibrosis that may be quite extensive.
SYSTEMIC EFFECTS OF INFLAMMATION • collectively called the acute-phase reaction, or the systemic inflammatory response syndrome • The cytokines TNF, IL-1, and IL-6 are the most important mediators of the acute-phase reaction • IL-6 stimulates the hepatic synthesis of a number of plasma proteins
SYSTEMIC EFFECTS OF INFLAMMATION 1- Fever: cytokines (TNF, IL-1) stimulate production of prostaglandins in hypothalamus. In the hypothalamus the PGs, especially PGE2, stimulate the production of neurotransmitters, which function to reset the temperature set point at a higher level 2- Production of acute-phase proteins: C-reactive protein, others; synthesis stimulated by cytokines (IL-6, others) acting on liver cells. Many acute-phase proteins, such as CRP and SAA, bind to microbial cell walls, and they may act as opsonins and fix complement, thus promoting the elimination of the microbes
3- Leukocytosis: cytokines (colony-stimulating factors) stimulate production of leukocytes from precursors in the bone marrow 4- septic shock (In some severe infections) : fall in blood pressure, disseminated intravascular coagulation, metabolic abnormalities; induced by high levels of TNF
6- anorexia, somnolence, and malaise: the actions of cytokines on brain cells 7- wasting syndrome called cachexia, which is mainly the result of TNF-mediated appetite suppression and mobilization of fat stores (only in severe cases)