Download
1 / 26
260 likes | 599 Views
Posterior Fossa Volume and Skull Base Geometry in Children with Chiari I Malformation. S.Sgouros Birmingham Children’s Hospital Birmingham, U.K. Acknowledgements. Kal Natarajan, Computer Scientist at the Neuroscience Informatics Laboratory Menia Kountouri, Research Fellow

E N D
Posterior Fossa Volume and Skull Base Geometry in Children with Chiari I Malformation S.Sgouros Birmingham Children’s Hospital Birmingham, U.K.
Acknowledgements • Kal Natarajan, Computer Scientist at the Neuroscience Informatics Laboratory • Menia Kountouri, Research Fellow • The Neuroscience Informatics Laboratory at ICH/BCH is supported by the Bernard Williams Syringomyelia Research Fund
Hindbrain Hernia – Chiari I • Hindbrain hernia is considered to be due to maldevelopment of the posterior cranial fossa leading to small volume • Geometrical studies of 2D sagittal projections and quasi 3D studies • Lack of systematic analysis in paediatric age group
1998-2007 a total of 82 children with isolated Chiari I, 61 operated, 21 asymptomatic Normal control group 70 children (1m-15y) Extensive range of 3D image analysis tools Included: Children with symptomatic Chiari I Complete set of MR scans Excluded: Craniosynostosis-related hindbrain hernia e.g. Crouzon’s Shunt prior to craniovertebral decompression 3D Morphometric Analysis of Chiari I
Aim of the Study • To establish whether the volume of the posterior fossa in children with Chiari I is smaller than normal controls, as has been previously postulated • To establish the correlation between posterior fossa volume and the development of syringomyelia
Patients • 42 children (24 Male, 57%) • Mean age: 127 m (range: 36-204 m) • Syrinx present pre-op: 25 patients (59%) • Comparison with 51 normal children of similar age
Method • Segmentation technique on pre-op MRI scans • Parameters measured: • Posterior Fossa Volume • Intracranial Volume • Posterior Fossa to Intracranial Volume ratio • Factor analysed: syringomyelia preop • One way ANOVA, graphic data analysis (LOWESS smoothing technique)
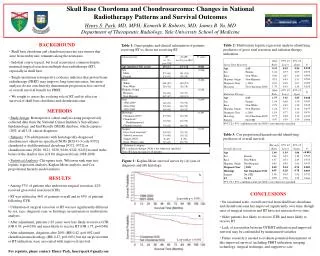
Results Normal CMI no syrinx CMI+syrinx (n=51) (n=17) (n=25) ICV (cm3) 1383 1459 1400 p=0.363 PFV (cm3) 186 196 171p=0.036 PFV/ICV0.135 0.134 0.122p=0.004
PFV in Chiari I • Two different varieties of Chiari I • Children with Chiari I without syringomyelia have normal posterior fossa volume • Children with Chiari I and syringomyelia have a smaller posterior fossa volume than normal
Aim of the Study • To establish whether the skull base in children with Chiari I is underdeveloped compared to normal controls, as it has been previously postulated • To establish the correlation between skull base geometry and the presence of syringomyelia
Patients • 30 children (17 Male, 57%) • Mean Age: 128 m (range: 36-204 m) • Syrinx present pre-op: 16 patients (53%) • Comparison with 42 normal children of similar age
Segmentation technique on pre-op T2w axial MRI scans: Angles Crista Galli - Dorsum Sellae - Foramen Magnum LT IAM - Foramen Magnum - RT IAM LT AC-CG-RT AC LT IAM - Dorsum Sellae - RT IAM Distances LT - RT IAM LT AC – RT AC Dorsum Sellae - Foramen Magnum Effect of syringomyelia One way ANOVA analysis Graphic data analysis Method
Results NormalChiari I/- syrinx Chiari I/+ syrinx CG-DS-FM 135° 145° 151°(p=.000) LT IAM-FM-RT IAM 110° 122° 123°(p=.001) LT AC-CG-RT AC 34° 29° 29° (p=.000) LT IAM-DS-RT IAM 96° 97° 101° (p=.394) LT IAM-RT IAM (mm) 58 75 63 (p=.000) LT AC-RT AC (mm) 32 3127(p=.001) DS-FM (mm) 46 5040 (p=.101) (p=.037, p=.009)
Skull Base Geometry in Chiari I • Chiari I overall have (in comparison to normal) : • longer anterior fossa • wider and steeper posterior fossa • and different slope / angle of clivus • Patients with syringomyelia have slightly different skull base geometry than those without
Conclusions • Chiari I + Syringomyelia: small posterior fossa volume • Chiari I – Syringomyelia: normal posterior fossa volume • Chiari I: all skull base structurally different from normal • Differences in skull base geometry in syringomyelia • Unlikely that the development of syringomyelia is an evolution in the natural history of Chiari malformation (difficult for posterior fossa to become smaller and geometry to change, as the syringomyelia develops, unless there is a primary skull base synostosis)
Possible Pathogenesis • Possible different pathogenesis for the two subgroups of the Chiari I • Chiari I – syrinx: single hit (mesodermal deformity) • Chiari I + syrinx: double hit (mesodermal deformity + cavitation) • Ab initio formation of syringomyelia “loss” of CSF in the spine smaller posterior fossa (analogous to open myelomeningocele) • Anterior fossa deformity secondary to posterior fossa mesodermal defect or primary malformation affecting all the skull base?
Syringomyelia 2007 • Major international conference on syringomyelia • Rugby, U.K. • October 23-26, 2007 • Abstract Closing Date: 30th June 2007 • www.syringomyelia2007.org