Download
1 / 15
250 likes | 1.28k Views
Erythema Multiforme. EM minor & EM with mucosal involvement. Self-limited, recurrent disease, usually in young adults No or only a mild prodrome (1 to 4 weeks) Sharply marginated erythematous macules become raised, edematous papules (24 to 48 hours) Periphery: ring of erythema

E N D
EM minor & EM with mucosal involvement • Self-limited, recurrent disease, usually in young adults • No or only a mild prodrome (1 to 4 weeks) • Sharply marginated erythematous macules become raised, edematous papules (24 to 48 hours) • Periphery: ring of erythema Central: flatters, more pruritic and dusky
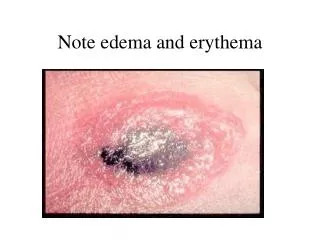
Classic EM lesion • “target” or “iris” lesion with three zones • Best observed on the palms and soles • Symmetrical and acral • Central dusky purpura • Elevated, edematous, pale ring • Surrounding macular erythema
Sites of Predilection • Dorsal feet • Extensor limbs • Elbows • Knees • Palms • Soles
Koebner’s phenomenon or photoaccentuation • Mucosal involvement in 25% -- usually limited to the oral mucosa • More severe classic case? Two or more mucous membranes involved in 45%
Steven-Johnson syndrome / EM major • Clinically different from minor • Frequently, febrile prodrome • Eruption occurs at all ages • Begins diffusely on the truck and mucous membranes • Flat, erythematous or purpuric macules incomplete “atypical targets” (may blister centrally) • Larger and more commonly confluent lesions compared to EM minor
Etiologic Factors • EM minor = herpes simplex infection • Typically orolabial • 1 to 3 weeks (10 day average) after herpes lesion • May or not follow herpes outbreaks • EM major(SJS) = medications • Most centrally accentuated eruptions with atypical targets • Sulfonamids, antibiotics, NSAIDs, allopurinol, anticonvulsants • Due to abnormal metabolism of medications
Etiologic Factors • Also, EM major = Mycoplasma pneumoniae • Prominent mucosal involvement and bullous skin lesions – NOT classic iris lesions • Resemble SJS cases • And, EM major = radiation therapy • With phenytoin and tapering corticosteroids – induces EM starting at radiation port
Pathogenesis • Activated T lymphocytes • Epidermis: cytotoxic or suppressor cells • Dermis: helper T cells • EM minor – specific HLA types (HLA-DQ3) • SJS – abnormalities in drug metabolism Hence, there is a genetic component for both diseases
Differential Diagnosis • Herpes simplex • Drug eruptions • Giant urticaria • Stevens-Johnson syndrome • Dermatitis herpetiformis