Download

1 / 18
490 likes | 2.27k Views
Erythema multiforme (EM). Definition. Erythema multiforme is a serious of acute, self-limited, recrudescent and inflammatory dermatopathy characterized by erythema, papula and blister, which involves of skin and mucosa. Etiopathogenisis.

E N D
Erythema multiforme (EM)
Definition Erythema multiforme is a serious of acute, self-limited, recrudescent and inflammatory dermatopathy characterized by erythema, papula and blister, which involves of skin and mucosa.
Etiopathogenisis 1. Hypersensitivity with infection: virus, mycoplasma, bacterium, mycetes or protozoon 2. Food allergy 3. Climatic change 4. Drug allergy (drug eruption) 5. Connective tissue diseases
Pathogenesis Possible mechanism is hypersensetivity of small vesseles to some sensitizers.
Clinical Manifestation 1. Lesions:erythema, papula, blister, bulla or blood bister. The mark lesion is iris-like lesion. 2. Distribution: Predilection sites include back of hand, dorsum of foot, face and cervix. Mucosa can be involved.
Idio-EM:etiology unknown Symptomatic EM:etiology known
Grouping:according to appearance Macule type Papule type Blister type
Macule Type Bright red edematous macule ,round or orbicular-ovate. The macule may expand peripherad with gloom prunosus center and ruby-red margin. If central edema is absorbed and depressed like a disk, the lesion will offer ring shape. Several ring-shape lesion may confluens together to polynucleation.
Papule Type It’s the most common type. Because of serosity exudation,the papule swell up to the surface of skin , dome shape and soybean size,sometimes like wheal.
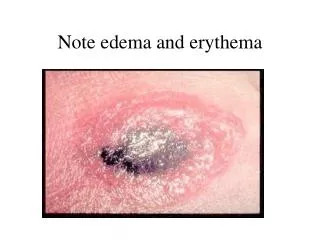
Blister Type Severe exudation. The center of rash is blister ,surrounding with kermesinus areola. It’s called iris-like lesion if different colors and sizes of loops overlapped,like iris. It is more serious when bulla or blood blister occur.
Mucosal Damage General damage is gray patch, then blister, erosion, bleed, ulcer and scab. When in eye, conjunctivitis is more frequent.
Histopathology Early lesions include dropsy of upper stratum of dermis, vasodilatation swell of vessel wall, and perhaps, fibrinoid degeneration. The dermal infiltrate is largely lymphocyte, eosinophile granulocyte, neutrophil. The blisters lie in the dermal-epidermal junction, or in basal cells.
Laboratory examination • Hemogram: anemia, leukocytosis (sometimes leukopenia ) ,eosinophile granulocyte increase • ESR: increase • Hemoculture: negative • Sometimes proteinuria and hematuria.
Diagnosis and Differential Diagnosis • Evidence for diagnosis: • 1. Pleomorphism • 2. Predilection: distal extremities and face, etc. • Both skin and mucosa could be involved. • EM must be distinguished from herpetiform dermatitis and pemphigoid.
Treatment Medication: 1. Search for reasons so that corresponding treatment can be given. Stop all doubtful allergized medicine. 2. The treatment of EM is determined by type, pathogenetic condition and diseased region. Antihistamine drugs are generally chosen. 3. In severe cases, systemic steroid combined with antibiotics may be used, even supportive care such as blood transfusion or high protein diet when necessary.
External: • Skin erythema , papula: calamine lotion or catapasm: • Bulla: suck the liquid • Erosion and effusion : hydropathic compress with 3%boric acid solution or Pow. Neomgcin-coal-tar. • Oral mucosa erosion: Rinse the mouth with 2% NaHCO3,then repaste Pow.Qingdai, Pow. Xilei, • Cream. mucosal Ulcer or dental ulcer film coating , etc. • 3. Ocular damage: Flush with NS,then apply oculentum acidi borici or Cortisone eyewater, etc. It is necessary to prevent conglutination, secondary infection ,corneal ulcer and perforation, etc.