Download
1 / 48
700 likes | 2.06k Views
Babak Saedi Associate Professor of Department of Otolaryngology Tehran University of Medical Sciences. Frontal Sinus Surgery. http://www.dr.babaksaedi.com/DesktopDefault.aspx?tabindex=14&tabid=115&lang=fa-IR. Anatomy. Uncinate process Agger Nasi.

E N D
Babak Saedi Associate Professor of Department of Otolaryngology Tehran University of Medical Sciences Frontal Sinus Surgery http://www.dr.babaksaedi.com/DesktopDefault.aspx?tabindex=14&tabid=115&lang=fa-IR
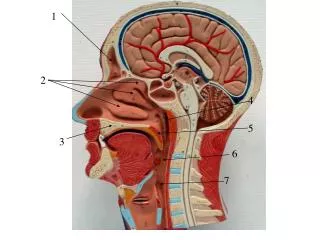
Anatomy • Uncinate process • Agger Nasi http://www.dr.babaksaedi.com/DesktopDefault.aspx?tabindex=14&tabid=115&lang=fa-IR
Anatomy • Cribriform Plate • Lamina papyracea • Fovea ethmoidalis
Uncinate Process Wormald PJ 2008
Anatomy A common reason for ESS failure is inadequate removal of cells obstructing the outflow of the frontal sinus
Single AggerNasi Cell Without Frontal Cells Wormald PJ 2008
Single AggerNasi Cell Without Frontal Cells Wormald PJ 2008
Single AggerNasi Cell Without Frontal Cells Wormald PJ 2008
Transition From Frontal Sinus To Frontal Recess Wormald PJ 2008
Frontal Cells Kuhn FA 1994
Frontal Cells • Type I - Single cell above the agger nasi • Type II - Two or more cells above the agger cell • Type III - Single cell extending from the agger cell into the frontal sinus • Type IV - Isolated cell within the frontal sinus
Surgical Indications • Chronic sinusitis unresolved with maximal medical therapy; • Polyps and allergic fungal sinusitis • Intracranial complications of sinusitis • Mucoceles or mucopyoceles • Benign neoplasms such as osteomas, inverting papillomas, or fibrous dysplasia.
Endoscopic Frontal Sinusotomy • Understand the patient’s frontal recess anatomy • Ascertain the anatomical reason for frontal recess/frontal sinus obstruction • Determine the best surgical approach to the problem
Endoscopic Frontal SinusotomyPrinciples • Dissection should be performed from posterior to anterior and from medial to lateral • Preserve all frontal recess mucus membrane • The frontal ostium can be stented or left alone!!!! Kuhn FA 2006
http://www.dr.babaksaedi.com/DesktopDefault.aspx?tabindex=14&tabid=115&lang=fa-IRhttp://www.dr.babaksaedi.com/DesktopDefault.aspx?tabindex=14&tabid=115&lang=fa-IR
Draf I • Anterior ethmoid cells • Uncinate process • Obstructing frontal cells
Draf II • Floor of the frontal sinus • Lamina papyracea to Septum • Anterior face of Frontal
Draf III • Modified Lothrop • Interfrontal septum • Nasal septum • Frontal sinus floor
Surgical Outcomes Following the EndoscopicModified Lothrop Procedure • Conclusion: EMLP is a safe and effective surgical alternative to OPF for patients with recalcitrant frontal sinus disease. Major complications are rare. A large percentage of patients may require revision surgery Laryngoscope, 117:765–769, 2007
Frontal Sinus Trephination • Finding the frontal recess • Mucoceles • Isolated Type IV frontal cells • With endoscopic techniques to assist with Draf II and III
Endoscopic Frontal Sinoplasty • The least invasive procedure • It can be used as a stand-alone procedure or with ethmoidectomy • It pushes the medial aggernasi cell wall laterally and the ethmoid bulla lamella posteriorly • K Kuhn FA 2006
Frontal Recess & Frontal Beak Wormald PJ 2008
Osteoplastic Flap Vs. Draf III • Narrow Nasal Airway • Small Frontal Sinus • Deep Nasion • Floor of sinus < 1.5 cm • Heavy thick nasofrontal beak • Proliferative osteitis, complicated chronic infection • Favor Draf III for mucoceles
The frontal osteoplastic flap: does it still havea place in rhinological surgery • The frontal osteoplastic flap still has a role in frontal sinus surgery. The Journal of Laryngology & Otology (2011), 125, 162–168.
May be modified to fit the patient Osteoplastic Flap
Osteoplastic Flap Approach • Osteoplastic and endoscopic (above and below approach) • Frontal sinus obliteration Wynn R, et al 2007
Riedel's Procedure • Osteomyelitis of the anterior wall of the frontal sinus • Failure of frontal sinus obliteration • Some tumors of the frontal sinus
Pearl #1 Carefully Examine the Anatomy in more than one CT plane • Size of the frontal recess • Size of the frontal sinus • Bony thickening or neo-osteogenesis • Identify the frontal sinus drainage pathway • Note the position of the anterior ethmoidal artery
Pearl # 2 Identify the Anterior Ethmoidal Artery • Superior extension of anterior wall of bulla • Nipple on the medial orbital wall • 1-4 mm’s below skull base • Typically posterior to supraorbital ethmoid cells
Pearl #3: Plan the least invasive approach possible • Ethmoidectomy with Middle Meatal Antrostomy without frontal recess surgery • Frontal recess surgery • Endoscopic frontal sinusotomy • Frontal sinus trephination • Unilateral extend frontal sinus surgery (Draf II) • Endoscopic Modified Lothrop (Draf III) • Osteoplastic flap with or without obliteration
Pearl #4 Positively Identify the Skull Base Posteriorly • Skeletonize from posterior to anterior • Open cells immediately posterior to the middle turbinate • Identify the sinus with a seeker
Pearl #5 Positively identify the frontal sinus with a probe • Need a relatively dry field • 45 degree telescopes are helpful • Identify medial orbital wall and stay close to it dissecting superiorly • Opening to frontal sinus typically medial • Identify opening with a probe
Pearl # 6 Preserve the Mucosa • Consider leaving polyps if sinus is open • Remove osteitic intersinus septae carefully • Do not traumatize unless sinus can be opened widely • Standard frontal sinusotomy • Draf Type II • Works well if you can: • Preserve mucosa • Remove bony partitions • Create an ostium >4-5 mm
Pearl #7 Keep the Sinus Open Postoperatively • Remove fibrin and blood from frontal recess and frontal sinus • Remove residual bone • Antibiotics, topical steroids? • Oral Steroids?
Conclusion • Very little evidence based medicine • Do the least invasive procedures first • Be aware of various surgical options • Image guidance a valuable tool • First do no harm