Download
1 / 29
310 likes | 2.95k Views
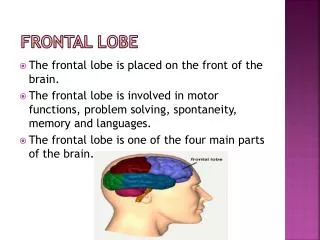
Naso-orbital Ethmoid and Frontal Sinus Fractures. Grand Rounds Presentation Jim C. Grant, M.D. Byron J. Bailey, M.D. FACS April 29, 1998. Naso-orbital Ethmoid Fractures Introduction. Suspect in Central Midfacial Trauma Failure of Diagnosis Leads to Significant Facial Deformities

E N D
Naso-orbital Ethmoid and Frontal Sinus Fractures Grand Rounds Presentation Jim C. Grant, M.D. Byron J. Bailey, M.D. FACS April 29, 1998
Naso-orbital Ethmoid FracturesIntroduction Suspect in Central Midfacial Trauma Failure of Diagnosis Leads to Significant Facial Deformities Isolation of Lower 2/3 Medial Orbital Rim Lateral Nose Medial Orbital Wall Nasomaxillary Buttress Frontal Process of Maxilla / Maxillary Process of Frontal Bone
Basic Principles in Craniomaxillofacial Management Early One Stage Repair Exposure of All Fracture Fragments Precise Anatomic Rigid Fixation Immediate Bone Grafting as Indicated for Bony Loss Definitive Soft Tissue Management
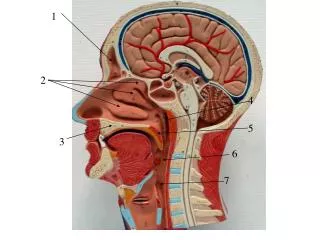
Naso-Orbital Ethmoid Region Bony Anatomy Limits of the Naso-orbital Ethmoid Region Horizontal Buttress Vertical Buttress -- “Central Fragment” Medial Orbital Wall Nasal Bones Ethmoid Labyrinth / Perpendicular Plate
Naso-orbital Ethmoid AnatomySoft Tissue Structures Medial Canthal Tendon Anterior / Posterior / Superior Limbs Function Nasolacrimal Collecting System Ensheathed Partially by Superior and Anterior Limbs Inferior Aspect Prone to Injury
Naso-orbital Ethmoid FracturesSigns and Examination Medial Canthal Tendon Displacement Traumatic Telecanthus (IC/IP > 1/2) Lack of Eyelid Tension -- Positive Bowstring Test Rounding of the Medial Canthus Shortened Palpebral Fissure
Naso-orbital Ethmoid FractureSigns and Examination Lacrimal System Inspect With Loupes if Laceration in Area\ Damaged Area Canulated Associated Ocular Injury Enophthalmos Diplopia Entrapment Vertical Dystopia Loss of Globe Integrity
Naso-orbital Ethmoid FracturesSigns and Examination Nasal Deformity -- “pushed between the eyes” Reduced Nasal Projection and Height Flattened Nasal Dorsum Septal Deviation / Dislocation Intracranial Involvement Cerebrospinal Fistula Pneumocephalus Frontal Sinus Involvement
Naso-orbital Ethmoid FracturesSigns and Examination Palpation of Nasal Bones Allows Assessment of Integrity of Dorsal Nasal Height Collapse Implies Absence of Support Click on Pressing Inward at the Medial Canthal Ligament Bimanual Examination
Naso-orbital Ethmoid FracturesClassification Type I-- Involves Single Segment Central Fragment Fractures Type II -- Comminuted Central Fragment With Fracture Lines Remaining Peripheral to the Medial Canthal Tendon Insertion Type III -- Comminuted Central Fragment With Fracture Lines Extending Beneath the Medial Canthal Tendon Insertion
Naso-orbital Ethmoid FracturesGoals of Management Reconstitution of the Skeletal Framework of the Naso-orbital Ethmoid Region Stabilization of the Intercanthal Width and Medial Canthal Tendons Orbital Reconstruction Establishment of Nasal Support Reconstitution of Other Craniofacial Injuries Including Frontal Sinus Soft Tissue Repair
Naso-orbital Ethmoid FracturesType I Incomplete Repair No Requirement for Superior Surgical Approach Inferior Approach via Gingivobuccal Sulcus Incision and Transconjunctival / Subciliary Reduction and Rigid Fixation at Inferior Orbital Rim and Pyriform Aperture
Naso-orbital Ethmoid Fractures Type I Complete Displaced Superior Fragment Requires Superior Approach via Coronal Flap With Reduction and Stabilization at the Superior Medial Orbital Rim Inferior Approach With Reduction and Stabilization at Inferior Orbital Rim and Pyriform Aperture Unless Severe Lateral Displacement --Transnasal Wiring Not Indicated
Naso-orbital Ethmoid FracturesType II Repair Repair Requirements Include: Transnasal Reduction of Medial Canthal Tendon-Bearing Bone Fragments Interfragment Wiring to Link All Fragments Rigid Fixation After Reduction Transnasal Wire Must be Placed Superior and Posterior to the Medial Canthal Tendon on the Central Fragment
Naso-orbital Ethmoid FracturesType III Repair Same Basic Principles of a Type II Repair Comminuted Fractures Not Suitable for Reconstruction -- Medial Canthal Tendon Detached Bone Grafts May Be Required Medial Canthal Tendon Secured To Second Set of Transnasal Wires -- Point of Attachment is Superior and Posterior
Naso-orbital Ethmoid FracturesNasal Support Repair Dorsal Bone Grafting Reduction of Septal Fracture Possible Use of Medial Crura Strut for Columellar Support Placement of Canilevered Graft Under the Dome
Naso-orbital Ethmoid FractureLacrimal System Repair Routine Exploration With Canalicular Probing Not Indicated Identifiable Disruption -- Canulate and Suture Only 5% Incidence of Cases Require DCR Later
Naso-orbital Ethmoid FracturesSoft Tissue Repair Padded Bolsters Placed Secured Through Transnasal Wiring Lack of Bolstering Leads to Thickened Skin in this Area Increasing the Intercanthal Soft Tissue Difference
Naso-orbital Ethmoid FracturesOrbital Repair Restoration of Orbital Volume and Contour Must be Addressed Use of Bone Grafts and Alloplastic Materials in the Orbital Floor
Naso-orbital Ethmoid FracturesComplications Persistent Telecanthus Anteriorly Placed Transnasal Wires Inadvertent Elevation of Tendon Inadequate Reduction and Stabilization of Central Fragment Lack of Adequate Repair of the Orbit Lack of Adequate Repair of Nasal Support Soft Tissue Thickness Secondary to Inadequate Bolstering
Frontal Sinus FracturesIntroduction Incidence -- 5 - 12% Craniofacial Injuries High Morbidity and Mortality Management Goals Avoidance of Early and Late Complications Cosmetic Reconstruction Progresses of Frontal Sinus Surgery
Frontal Sinus FracturesAnatomy Frontal Sinus Development Anterior versus Posterior Table Nasofrontal Duct Arterial / Venous Blood Supply Sensory Innervation
Frontal Sinus FracturesDiagnosis Physical Examination Assess for Associated Ocular Injuries Assess for Associated Intracranial Injury Assess for Associated Craniofacial Injury -- Naso-orbital Region CT Scanning Difficult to Assess Patency of Nasofrontal Duct
Frontal Sinus FracturesSurgical Approaches Frontal Sinus Trephination Frontoethmoidectomy Osteoplastic Flap -- Most Commonly Employed Frontal Craniotomy
Frontal Sinus FracturesOperative Indications Anterior Table Displacement With an Aesthetic Forehead Deformity Nasofrontal Duct Involvement / Obstruction Displaced Posterior Table Fractures
Frontal Sinus FracturesAnterior Table Fractures Nondisplaced Anterior Table Fracture Displaced Anterior Table Fracture Status of Nasofrontal Duct Sinus Preservation Sinus Obliteration Removal of Mucosa NF Duct Obstruction Sinus Packing
Frontal Sinus FracturesNasofrontal Duct Reconstruction Intersinus Removal Allowing Drainage Through Contralateral Duct Placement of Catheter Through Traumatized Nasofrontal Duct Frontoethmoidectomy Approach When Posterior Table Not Requiring Repair
Frontal Sinus FracturesPosterior Table Repair Nondisplaced Posterior Table Fractures Minimally Displaced Posterior Table Fractures-- Less than One Width Displaced Posterior Table Fracture Nasofrontal Duct Status Cerebrospinal Fluid Leak Degree of Comminution
Frontal Sinus FracturesCranialization Coronal Incision -- Osteoplastic / Frontal Craniotomy Preservation of Anterior Pericranium Intersinus Septum Removal / Posterior Table Removal Debridement of Necrotic Tissue / Repair of Dural Tears Sinus Mucosa Removal Nasofrontal Duct Obliteration Interposition Pericranial Flap to Floor