Download
1 / 14
140 likes | 174 Views
Learn about human thyroid gland development from embryogenesis to congenital hypothyroidism, including control factors and diagnostic methods. Understand the clinical presentation, maternal factors, and treatment guidelines.

E N D
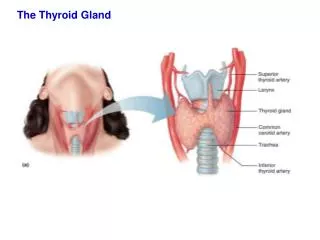
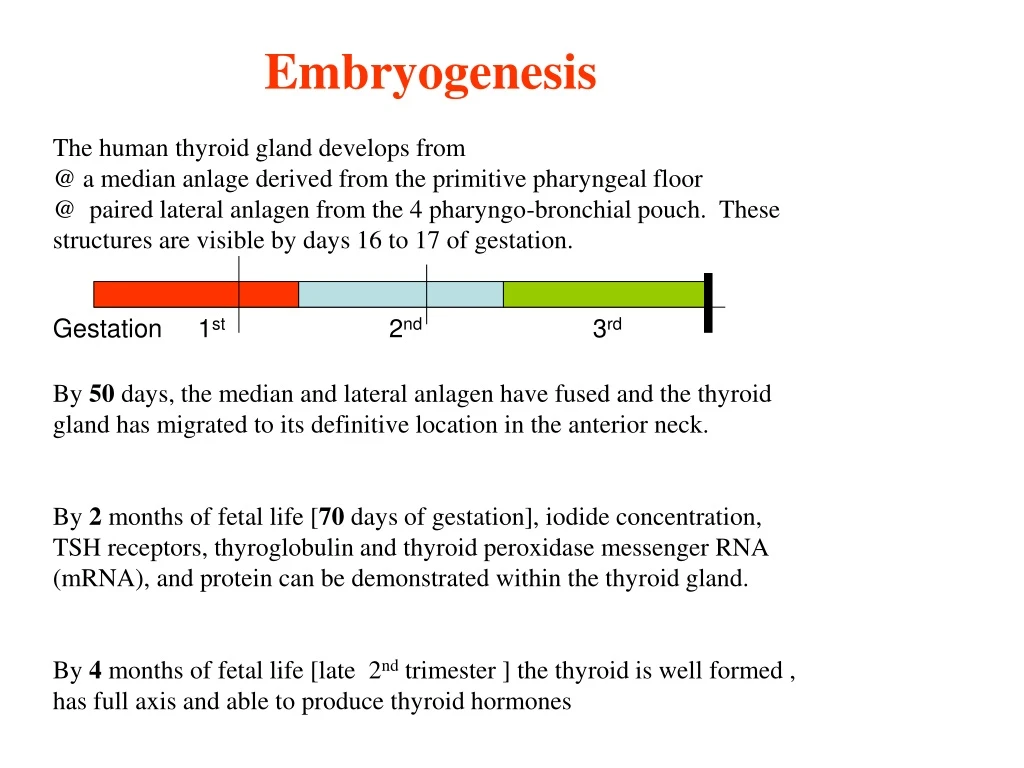
Embryogenesis The human thyroid gland develops from @ a median anlage derived from the primitive pharyngeal floor @ paired lateral anlagen from the 4 pharyngo-bronchial pouch. These structures are visible by days 16 to 17 of gestation. By 50 days, the median and lateral anlagen have fused and the thyroid gland has migrated to its definitive location in the anterior neck. By 2 months of fetal life [70 days of gestation], iodide concentration, TSH receptors, thyroglobulin and thyroid peroxidase messenger RNA (mRNA), and protein can be demonstrated within the thyroid gland. By 4 months of fetal life [late 2nd trimester ] the thyroid is well formed , has full axis and able to produce thyroid hormones Gestation 1st 2nd 3rd
What control Thyroid embryo genesis ? Thyroid embryogenesis is dependent on production of a programmed sequence of homeobox and transcription factors : @ TTF-1 ,2 [thyroid transcription factors 1 and 2} @ PAX-8. Targeted mutation in mice TTF-1 -----------Thyroid gland aplasia TTF-2 --------- Ectopic, sublingual thyroid gland. PAX-8 -------- Hypolasia (very small thyroid gland ) Mutations in these genes, however, account for only approximately 2% of human thyroid dysgenesis.
1-Congenital hypothyroidism • Prevalence • Worldwide 1: 4,000 infants • Hispanics /Native Americans 1 : 2,000 • Black Americans 1 : 32,000 • Male : Female 1:2
Screening for congenital hypothyroidism Mental retardation due to Congintal hypothyroidism is preventable 1. Methods used 2 methods are currently avaliable Primary TSH [+ FT4] Primary T4 [+ TSH] Picked up > 98 % of primary CH Picked up all Miss rare cases of 2nd , 3rd CH - Miss cases with delayed rise TSH - 2. Timing , the best is at 2-3 post delivery [ not practical in many countries] TSH Mu/l < 30 > 30 but less < 60 > 60 do FT4 in same sample CH Normal Normal Low Investigate + Rx Reapt TSH +FT4
Primary Hypothyroidism A. Defect of fetal thyroid development Aplasia, ectopia (dysgenesis) B. Defect in thyroid hormone synthesis (e.g., goitrous hypothyroidism) 1. Thyroid oxidase mutations: Permanent (homozygotic) Transient (heterozygotic) 2. Iodide transport defect 3. Thyroid peroxidase defect 4. Thyroglobulin synthesis defect 5. Deiodination defect C.Iodine deficiency (endemic goiter) Neurologic type Myxedematous type D. Maternal Factors 1. antibodies TSH receptorblocking antibody (TRBAb) Other name TSH binding inhibitor immunoglobulin) 2. Maternal medications Propylthiouracil Methimazole Amiodarone 3. Radioiodine, iodides dyshermogensis
Clinical presentation – if not picked-up by screening 1. Laboratory errors 2. Rare cases delayed rise in TSH 3. Bay attention to identical twins transfusion of euthyroid blood from the unaffected twin normalized the serum level of T4 and TSH in the affected twin at the initial screening. 4. all neonate asymptomatic at birth Aim to diagnose as early as possible Growth parameters : Birth weight & length are normal but what about head size ? Prolongation of physiologic jaundice –why ? Feeding difficulties : sluggishness lack of interest somnolence choking spells during nursing poor appetites Respiratory difficulties : Apneic episodes Noisy respirations Nasal obstruction First month
Constipation (Difficult to treatment). Anemia is often present and is refractory to treatment with iron What type of anemia ? Physical Examinations : IF early can be essentially normal In long-standing untreated The temperature is subnormal, often less than 35°C The face may suggest diagnosis protruded tongue (minimal initially) The abdomen is large Umbilical hernia is usually present. Skin of limbs cold & mottled. Edema of the limbs & genitals CVS examinations may show : The pulse is slow Heart murmurs Cardiomegaly Asymptomatic pericardial effusion . Because symptoms appear gradually, the diagnosis is often delayed. Common finding But commonly overlooked
Diagnosis of primary hypothyroidism is straight forward Step 1 Confirm diagnosis Thyroid function test FT4 TSH Step 2 identify the cause Clinical clue --- mass at base of the tongue thyroglossal cyst (be careful) Thyroid scan (123 I-sodium iodide ) Try to localize the gland Ectopic Normal position Not visualized with increase radioactive aplasia TRAB I-Trapping defect AR USS thyroid present Sporadic Rx (life) Autosomal Recessive Rx (life) Aplasia Rx TRAB
Treatment Guide lines Start treatment as possible early mean Idealy < 2 weeks but < 6 week is ok Start 8 micg/kg/dose [once dialy] l-thyroxine is tablet thus embrically use 37.5 micg l-thyroxine once daily or embrically use 50 micgs Reapt the TFT after 2 weeks where most infant normalize FT4 Aim to keep FT4 at the upper half of normal . TSH may still elevated , ignore as far FT4 is in the target range Follow-up : At 2 , 4 weeks of start Every month for frist 6 months Every 2 months for the the rest of year Every 3 month till age 3 years Every 4 month till growth & puberty completed Every 2 weeks if you change the dose More frequents if there is concern about the compliance
Infant treated at age < 6 weeks and maintained normal FT4 in first 3 years of age their IQ=Normal
Thyroid in older children and Adults 1-Symptoms & Signs Thyroid hormone disturbance - due to deficiency or excess circulating thyroid hormone Under-Secretion-Hypo-( ) Over-secretion(Hyper-) ( ) General Lethargic “cool”“Fatigue” due to irritability , Nervousness Environment Cold intoleranceHeat intolerance Sleep Excessivelittle sleep “Insomnia” Bowel habit ConstipationDiarrhoea “Increased bowel movements” Skin Cold, dry skinWarm , moist skin Face peri-orbital puffinessExophalmos , Lid lag Weight GainLoss CVS - ? Slow H.RRapid Heart Rate ! Palpitations Pulse weak , small volume Rapid bounding Hands Cold , dryMoist ,Trembling hands Lower Limbs Cold Drypre-tibial myxoedema Muscle strength Weakness (proximal)Weakness (proximal) Symptoms Symptoms Symptoms Symptoms Symptoms Symptoms Symptoms Signs Signs Signs Signs Signs
2-Neck Mass and its effect • Thyroid enlargement (goitre) • It can be diffuse (generalised) and involve both thyroid lobes, or it can be more focal, as in nodular thyroid disease. • Patients and/or their relatives often notice a goitre as the first of a thyroid problem swallowing problems (dysphagia) 3-Extreme presentation Myxoedema coma Thyroid storm
Examine the Eyes ---- Look for * Proptosis (exophthalmia) --- examine from lateral view ------ Hyperthyroidism * Lid retraction – if you can see the upper part of sclera ------ Hyperthyroidism * Lid lag ---- by examination Move you finger from up-to-down Observe for upper lid lags behind ---- Hyperthyroidism Additional examinations A- Hand examination Examine the palmar Skin : Moist -------- Hyper Dray skin ---- Hypo Palmer erythema ---- Hyper Examine the Nails ---- clubbing ---- acropathy ------Grave’s (hyperthyroidism) Graves’ acropachy there is digital clubbing, thickening of the skin of the digits Examine for tremor – extend the hands / Paper Examine the Pulse - Low pulse ----- hypo ---- bradycardia - Rapid pulse ---- hyper-- tachycardia - Irregular ------- (atrial fibrillation) ---- not in exam) B- Muscle (upper /lower) examination looking for proximal myopathy for upper limp ask patient to rise his both arms above head for lower limp ---- ask patient to stand up C. Examination lower limp for pretibial myxoedema (Graves' dermopathy, thyroid dermopathy) 1-5%. Examination reflexes Slow / absent reflex -------- Hypothyroidism Hyper-reflexes --------------- Hyperthyroidism
Overall Approach to thyroid a thyroid problem can be rationally determined and subsequently managed by combining: • the history • clinical thyroid assessment • measurements of blood thyroid hormone levels • antibody studies; Anti-microsmal antibodies anti-thymoglobulin antibodies • thyroid imaging • thyroid technetium nuclear medicine scan • thyroid ultrasound • Fine needle biopsy