Download
1 / 57
570 likes | 699 Views
Recognition and Management of Pre-skin Cancer. Dr Vanessa Good GP White Horse Medical Practice Speciality Doctor Dermatology, Great Western Hospital. Pre-skin cancer in general practice. Is it relevant? How does it affect us?. Incidence of skin cancer is rising. How does this affect me?.

E N D
Recognition and Management of Pre-skin Cancer Dr Vanessa Good GP White Horse Medical Practice Speciality Doctor Dermatology, Great Western Hospital
Pre-skin cancer in general practice • Is it relevant? • How does it affect us?
How does this affect me? • Present to GP • Undifferentiated lesions • Referral pressures
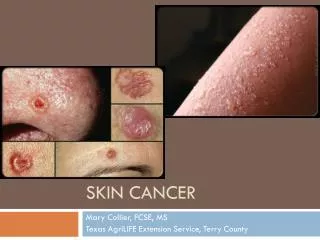
BOWEN’SDISEASE ACTINICKERATOSES
OBJECTIVES Increase confidence in • Recognition of Bowen’s and actinic keratoses • Treating within primary care • Knowing when to refer
Red scaly patch – what is it? • Bowens Disease • Superficial BCC • Tinea • Discoid Eczema • Psoriasis • other
History clues • Age • Growth rate • Lesion itchiness • Response to previous treatments • Dermatological history • Sun exposure history
History Red Flags PATIENT FACTORS • Older • Previous skin cancer • Significant UV exposure • Immunosuppression LESION FACTORS • Not itchy • Unresponsive steroids • Persistent growth
Examination clues • Location • Number of lesions • Edge • Texture • Scale • Crusting
LOCATION Bowens Superficial BCC Psoriasis Discoid Eczema
EDGE BOWEN’S DISEASE SUPERFICIAL BCC TINEA PSORIASIS ECZEMA
EDGE BOWEN’S DISEASE SUPERFICIAL BCC TINEA PSORIASIS ECZEMA
EDGE BOWEN’S DISEASE SUPERFICIAL BCC TINEA PSORIASIS ECZEMA
EDGE BOWEN’S DISEASE SUPERFICIAL BCC Centrifugal clearing TINEA PSORIASIS ECZEMA Raised marginated edge
EDGE BOWEN’S DISEASE SUPERFICIAL BCC TINEA PSORIASIS ECZEMA
EDGE BOWEN’S DISEASE SUPERFICIAL BCC TINEA PSORIASIS ECZEMA
TEXTURE PSORIASIS TINEA DISCOID ECZEMA ECZEMA
TEXTURE PSORIASIS TINEA DISCOID ECZEMA ECZEMA
TEXTURE PSORIASIS TINEA DISCOID ECZEMA ECZEMA
TEXTURE PSORIASIS TINEA DISCOID ECZEMA ECZEMA
TEXTURE PSORIASIS TINEA DISCOID ECZEMA ECZEMA
SCALE PSORIASIS TINEA
Superficial BCC CRUST
Guidelines for the management of Bowen’s Disease: 2006 UpdateBritish Association of Dermatology • No one treatment superior for all cases • 10% recurrence rate • Size, wound healing, number of lesions relevant • Consider patient factors • Consider doctor factors • Follow up in 3 months
History Clues • Age • Growth rate • Pain or tenderness • Bleeding • Sun exposure history • Dermatological history • Other risk factors • Social history
Examination clues • Location • Skin appearance • Lesion features including: • Base • Induration • Ulceration
Is it a squamous cell cancer? INDURATION ULCERATION
RED FLAGS PATIENT FACTORS • Immunosuppression • Previous skin cancer • Previous PUVA LESION FACTORS • Rapid growth/evolving • Tenderness/ pain • Ulceration /bleeding • Raised base • Induration • Lips • Poor treatment response
Should I treat actinic keratoses? • 15-25% spontaneous regression per year • SCC transformation <1 in 100 per lesion /yr • 10 lesions, 14% risk invasive SCC in 5 years • Cannot predict invasive behaviour • Monitoring an option – informed choices • Treat high risk patients
Treatment choices • Emollients / keratolytics/ sunblock • Diclofenac 3% gel ( Solaraze) • 5-fluorouracil cream (Efudix) • Imiquimod ( Aldara) • Cryotherapy • Curettage and cautery/ excision • Photodynamic therapy – secondary care only
Which treatment to use? • Isolated lesion or multiple? • Location • Thick or thin? • Patient preference
What to tell your patient? • Sun damage • Risk of developing skin cancer • Changes to be concerned about • Sun protection measures • Emollients • Treatment options • Patient information leaflet and website info • Treatment information leaflet
Cryotherapy • Quick, economical, well tolerated • 70-75% clearance with 2 freeze-thaw cycles • 5-10 sec FTC • Risks: hypopigmented macular scar, inflammation, blistering • Reduce keratin first – an insulator • Poor healing in tibial area