Download
1 / 49
500 likes | 1.15k Views
Anesthesia for Orthopedic Surgery and Evoked Potentials Monitoring. Jampierre Mato CRNA,MSN,ARNP Clinical Adjunct Professor Anesthesiology Nursing Program Florida International University. The Specialty.

E N D
Anesthesia for Orthopedic Surgery and Evoked Potentials Monitoring Jampierre Mato CRNA,MSN,ARNP Clinical Adjunct Professor Anesthesiology Nursing Program Florida International University
The Specialty • Orthopedics has grown immensely within the past 2 to 3 decades, mainly due to the development of arthroscopic equipment and hardware to replace joints • Total joint replacement (shoulder, elbow, wrist, hip, knee, and ankle)-may offer a vast improvement in quality of life • Inter-vertebral disc replacements are now being offered • Benefits of arthroscopy • Much less invasive than open techniques • Allows direct visualization and manipulation with specialized equipment • Reduced discomfort and length of stay (many procedures done as outpatient)
Tourniquets • Pneumatic Tourniquets • Provide virtually bloodless field • Cuff should overlap only 3 to 6 inches • Area underneath must be padded and wrinkle-free • Overlap of cuff should be opposite of neurovascular bundle (e.g. on the humerus, overlap is on the lateral aspect-opposite the brachial plexus) • Inflation pressure usually 100mmHg greater than systolic blood pressure
Tourniquets Must exsanguinate extremity prior to inflation (elevate or use Esmarch bandage) Elevation is preferred in infected extremities Inflation pressures • Should not exceed 300mmHg in upper extremities • Should not exceed 500 mmHg in lower extremities
Tourniquet Pain Compression of intra-neural blood vessels • Causes secondary nerve ischemia • Leads to stimulation of pain pathways • Onset 45-60 minutes after inflation • Similar to thrombotic vessel occlusion • Activation of C fibers – burning and aching • Activation of A delta fibers – pins and needles • Difficult to treat, once it begins: analgesics and anesthetics have little effect, may need to treat sympathetic activation (tachycardia and hypertension)-What is the only true treatment?
Tourniquet Safety -Always place cuff where nerves are best protected in the musculature -Check proper function of machine -Never inflate for longer than 2 hours: 10 to 15 minute reperfusion interval required prior to re-inflation -Minimally effective pressure to occlude blood flow -Put display where you can see it • Report 60 minutes, then 15 min increments after that to the surgeon and be sure to chart that you did so • Always chart times on your record
Hip Surgery -ORIF – Open Reduction with Internal fixation • Done for fractures (usually frail/elderly) • Requires use of special fracture table (legs split with traction applied) • Frequent concomitant diseases (dementia, Parkinson’s, CAD, diabetes, etc.) • Frequently dehydrated • Occult blood loss can be significant • Intracapsular • Subcapital, transcervical – less blood loss • Extracapsular • Femoral neck, intertrochanteric, subtrochanteric – expect higher blood loss -Bipolar hip replacement (not a total hip arthroplasty): -done when fracture is not amenable to permanent fixation - femoral head and partial femoral neck are resected and replaced with a prosthesis -acetabular component is not fixed to the acetabulum -procedure usually takes less than an hour
Bipolar Hip Prosthesis • Cup is not attached to acetabulum • Utilized when patient will be non-ambulatory or will limit weight-bearing activities on hip for the rest of his life
Fat Embolism • High correlation with long bone, hip, and pelvic fractures • Occurs, to some degree, in all hip fracture patients • Patients typically have low oxygen saturation and low-grade fever • Fat Embolism Syndrome • Presents within 72 hours of injury • 3 hallmark signs: confusion, dyspnea, petechiae • Fat globules released into the blood through tears in medullary vessels • Theory that chylomicrons result from aggregation of circulating fatty acids • Thrombocytopenia and prolonged clotting times may occur
Fat Embolism Under GA • Diagnosing fat embolism syndrome under general Anesthesia • Decline in end tidal CO2 • Decline in arterial oxygen saturation • Rise in pulmonary artery pressures • Ischemic-appearing ST segment changes • Right sided heart strain • If severe, may lead to RVOT obstruction with resultant CV failure/arrest
Anesthetic Choice in Hip Fracture • General or Regional? • Extensively evaluated • Regional has lower mortality in the first 2 months post surgery • No significant difference in mortality after 2 months • General is associated with more thrombo-embolic events than regional • Morbidity post-general is higher immediately post operatively
Total Hip Arthroplasty -Usually done in lateral decubitis position • Higher degree of visibility and range of motion -Most common indication is Osteoarthritis (OA) AKA Degenerative Joint Disease (DJD) -Surgical Concerns (large incision, muscle trauma): • Acetabulum and femoral head/neck are very vascular • Resection of femoral head and neck • Reaming of femoral shaft to accept stem • Reaming of acetabulum to accept cup • Three life threatening complications • Bone cement implantation syndrome (cement rarely utilized in primary arthroplasty) • Peri-operative hemorrhage • Thrombo-embolism
Cement Implantation Syndrome Methylmethacrylate (MMA) • Mixing Powder and liquid causes exothermic reaction • Reaction causes expansion of cement and forces fat, blood, and air into the femoral venous channels • Residual monomer (liquid) is a potent systemic vasodilator and pulmonary vasoconstrictor • Release of tissue thromboplastin may trigger thrombo-embolism and cause hemodynamic instability
Total Hip Replacement *Minimally invasive/muscle sparing techniques are in widespread use
Closed Hip Reduction • May be necessary if prosthesis dislocates • Often done with heavy MAC or IV general with short-acting muscle relaxant, unless contraindicated • Extremes of flexion and internal rotation can dislocate a new prosthesis- abduction pillow is placed immediately post-operatively to avoid dislocation • Repeated dislocation of a hip prosthesis may require revision of the prosthesis-this is usually a failure of either surgical technique or the implant itself
Lateral Decubitus Position Used in thoracic, renal, and orthopedic procedures • Presents unique challenges to the anesthetist • Importance of body alignment (cervical/thoracic/lumbar) • Use of bean bag, axillary roll, pillows, sandbag • Cardiovascular Considerations • Respiratory Considerations • FRC decreased • Ventilation/Perfusion mismatch • Atelectasis • Use of PEEP (may worsen mismatch)
Total Knee Arthroplasty • Usually done for osteoarthritis or late-stage rheumatoid arthritis • Supine position • Regional vs. general anesthesia • Cement implantation syndrome (when is this a concern?) • Tourniquet concerns (ensure it is working) • Autologous blood donation • Bleeding is usually an issue post-op (once tourniquet is down)
Revision Joint Replacements • Previous joint replacements may need to be revised • Lifespan of current implants is postulated to be 10 to 15 years (may be shorter or longer, depending on recipient use) • Revision procedures tend to be lengthy and bloody • Intra-operative cell salvage is usually recommended • Infected joints need to be removed, with placement of antibiotic spacers until infection resolves-don’t use cell savage in suspected infection cases
Spinal Surgery -Done for a variety of diagnoses -herniated discs -spondylolisthesis/spondylosis -spinal canal stenosis -radiculopathy -myelopathy -osteophyte compression -scoliosis -kyphosis -post-traumatic stabilization
Common Diagnoses in Spine Surgery • Intervertebral disc herniation • Herniated disc may impinge on nerve roots and the cord itself • Spinal stenosis • Refers to narrowing of the spinal canal, for whatever reason (herniation, degenerative disc disease, spondylolisthesis, osteophyte formation, etc.)
Minimally Invasive Spine Surgery • Traditional spinal surgery (laminectomy, fusion, etc.) • Large incisions • Large amount of blood loss and prolonged wound healing • Great post-operative discomfort • Lengthy hospital stays • Commonly required anterior approach for the lumbar spine (laparotomy incision) • Mini-invasive spine surgery • Small incisions • Decreased blood less and faster wound healing • Decreased post-operative discomfort • Shorter hospital stay • Allows more complex procedures to be performed at once • Often allows access to lumbar spine that formerly required laparotomy
Mini-Invasive Spine Procedures • Lateral interbody fusion (LIF): • Allows complete lumbar discectomy and cage placement/fusion through a small flank incision • Trans-foraminal lumbar interbody fusion (TLIF): allows near-total discectomy with cage placement/fusion through a para-spinous incision • Axia Lumbar Interbody fusion (AxLIF): • Allows fusion of the L5-S1 interspace through a sub-sacral incision • Micro-discectomy: allows removal of a herniated portion of disc through an access port (may utilize microscope) • Laminectomy: allows for total or hemi-laminectomy through a port
Scoliosis • Lateral curvature of the spine • 75-80% of cases are idiopathic • Untreated, can lead to complex deformity • SSEP and MEP monitoring • Preoperative evaluation (cor pulmonale, pulmonary physiology changes) • PFTs, ABGs, EKG • Increased incidence of MH if caused by muscular dystrophy (in pediatric patients)
Scoliosis Surgery • Gold standard is multi-level fusion with instrumentation/rods • Potential for large blood loss (weighing of laps/sponges and tight I & O recording)- cell salvage usually utilized • “Wake up” test is uncommon, due to modern monitoring of evoked potentials • Severe respiratory disease may exist preoperatively, may be left intubated postoperatively • Major concerns with positioning (may have severe deformities) • Posterior, anterior, or thoraco-abdominal approaches may be necessary • May require double lumen tube if utilizing anterior thoracic approach
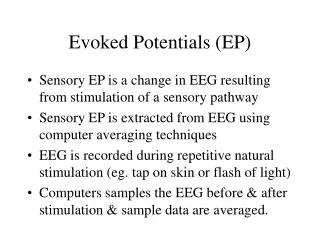
Monitoring of Evoked Potentials • Types: MEP, SSEP, EMG, VEP, BAEP • Indications: • Evaluation of pathology • Monitoring during any procedure which may compromise a nerve pathway
Cuneatus and Gracilis Tracts • Part of the dorsal-lemniscal sensory system • Responsible for touch, pressure, and vibration sensation • Located in the dorsal cord • Integrity of dorsal tract is assessed by SSEP monitoring (somato-sensory evoked potentials) • Sensations ascend on the ipsilateral side of the cord and cross into the contralateral side at the thalamus (considered a direct pathway to the cerebral cortex) • Procedures that may require SSEP monitoring: cerebral aneurysm clipping, spine surgery, CEA (questionable applicability), complex thoraco-abdominal aneurysm repairs (MEP’s are more useful since ischemia usually occurs in the ventral horn)
Reticular Activating System • Considered a secondary way by which sensory information arrives at the cerebral cortex • Deactivated during sleep • General anesthetics produce their effects through action on the RAS
Cortical Pathways • SSEP’s are recorded from the scalp • A peripheral nerve (ulnar/median or tibial) is stimulated, bilaterally, to procedure a potential that is recorded in the scalp • Stimulating electrodes are peripheral and detecting electrodes are central (the scalp)
Evoked Potential Waveforms • Amplitude: height of the waveform • Latency: can be thought of as the frequency • Decreased amplitude and/or increased latency indicate a compromise in nerve potential transmission • Factors that affect waveforms: temperature, PaO2, PaCO2, systemic blook pressure • VEP’s are most affected by our anesthetics, SSEP’s are moderately affected, and BAEP’s are marginally affected
Anesthesia During Evoked Potentials Monitoring • What can we do? • Maintain normothermia • Maintain blood pressure within 20% of baseline (critical in long-standing hypertension and/or small vessel disease)-consider invasive monitoring in select patients • Use anesthetics with minimal effects on waveform character (TIVA) • Maintain oxygenation (may be difficult during one-long ventilation) • Maintain normocapnea
The Ultimate Test of Nerve Pathway Integrity? • Wake up and move everything!
Foot and Ankle Surgery • Ankle fracture • Plate and screws • Bunionectomy • Hammer toe correction • Plantar fasciotomy • Achilles tendon repair
Ankle Block • Frequently used in podiatric cases • Insert needle lateral to the posterior tibial artery at the superior aspect of the medial malleolus (posterior tibial nerve) • Inject 5ml of local and 2ml as you withdraw the needle • Insert needle at the lateral border of the achilles tendon with the line between the malleoli, advance toward the lateral condyle, inject 5ml of local (sural nerve)
Ankle Block Technique • Draw a line between the superior edge of the medial malleolus across the anterior portion of the ankle • Flex the foot and place the needle between the tendons medial to the big toe (deep peroneal nerve), inject 5ml of local • With the remaining local, fan inject across the same plane across the ankle (saphenous nerve)
Upper Extremity Procedures -Usually amenable to brachial plexus block (interscalene, supraclavicular, axillary) Shoulder arthroplasty or arthroscopy • Requires beach chair/sitting position • Venous air embolism precautions • Airway concerns • Cardiovascular considerations? • Elbow arthroplasty or arthroscopy • Prone position • Turn head away from field • Turn table 90 degrees
Shoulder Arthroplasty Painful!!
Hand Surgery • Hand surgery • General vs. regional • Bier block • Axillary block • Wrist block • Tourniquet concerns • Long cases • Often awake, often uncomfortable (consider general)