Download
1 / 90
920 likes | 2.11k Views
Common Drugs - Dosing and Monitoring . Toxic? Me? With My Therapeutic Window?. PHENYTOIN. Introduction.

E N D
Common Drugs - Dosing and Monitoring Toxic? Me? With My Therapeutic Window? PHENYTOIN
Introduction This module is designed to help with your learning around some common drugs which you will be prescribing during your FY1 and FY2. As with many of the drugs we prescribe they are potentially very dangerous, are commonly mis-prescribed and there remains a mythology around them which lead to many of the errors associated with their use. Indeed the mere mention of these drugs on a ward round or in a clinic is often enough to bring even the most confident medic to their knees! By completing this module you should achieve a level of competence and safety which will mean you need rarely worry about them ever again. But if you are worried – you can always log on and re-do the module!
Aims and Objectives By completing this module you should be able to • appropriately prescribe gentamicin, digoxin, warfarin, heparin, Insulin, steroids and phenytoin • monitor drug therapy by taking appropriately timed drug levels for gentamicin, phenytoin, digoxin and warfarin • write up an IV insulin sliding scale and insulin infusion • convert a patient from IV insulin to regular subcutaneous dosing • appropriately prescribe anticoagulation intravenously, subcutaneously and orally. • recognise the common side effects and toxicity of gentamicin, warfarin, digoxin, phenytoin and steroids. • institute appropriate management to deal with toxic and other side effects
Challenging practice A 78 yo woman presents in A&E with severe urinary sepsis. She has hypertension but is otherwise fit and well. She is on Bendrofluazide 2.5mg od. Her U+Es are Na+131mmol/l, K 3.5+mmol/l Urea 13.8 mmol/l, Creatinine 127µmol/l. (1) Prescribe a stat dose of gentamicin. (2) When would you check the levels around the next dose? (3) How long will you continue the gentamicin?
Gentamicin Indications • Principally used against clinically significant gram negative sepsis – E. Coli, Proteus, Klebsiella, Pseudomonas (Tobramycin may be preferred for pseudomonas infection) • Some anti-Staphylococcal effect (but is commonly used in combination with other anti staphylococcal agents) • Also used in eye and ear infections (see introductory slide!) Why do we need to monitor? • Like many of the drugs in this module, gentamicin has a narrow therapeutic window (NTW) which means toxicity, particularly ototoxocity and nephrotoxicity, can be a serious complication of treatment.
Gentamicin Dosing - I • Previously (on ER) Gentamicin was given (a) In relatively small, standard doses to all patients regardless of weight, age and renal function i.e. 80 mg TDS regime (b) Often over inappropriately ‘long’ periods e.g. 7 days • This led to toxicity; Particularly when levels were unavailable / not done!
Gentamicin Dosing - II • Now superseded by dosing with initial ‘Big Bolus’ dose (see next slide) (Max 400mg total) Measure trough LEVELS after approx 12 hrs • Then depending on indications and patient Further ONCE a day dosing • Generally not given for longer than 3 – 5 days unless exceptional circumstances e.g. endocarditis • In endocarditis and pregnancy - The same dose (i.e. the once a day dosing) is split into BD or TDS regime • NB – A wise person once pointed out to me that one should be very wary of giving ototoxic drugs to blind people – It is not an absolute contraindication but think about this!
Gentamicin Dosing – Rule of Thumb Normal creatinine clearance - Gentamicin Dose 3 – 5 mg / kg Reduced creatinine clearance – Gentamicin Dose 1 – 2 mg /kg The following formula can be used to calculate creatinine clearance in order to determine the doses and dosing interval when prescribing gentamicin. Creatinine clearance (ml/min) = (N - age (years) ) x Wt (kg) serum creatinine (µmol/l) Where N = 150 for female patients; 160 for male patients >70 years,170 for male patients <70 years This does rely on you knowing or guestimating patient’s weight correctly – always err on the side of caution! • Normal creatinine clearance is (male range 97 – 137ml/min) and (female range 88 – 128 ml/min) i.e. approximately 100ml/min • It decreases with age (by approx 1ml/min/year from aged 20yo), reduced lean body mass i.e. reduced muscle mass, gender (as above) and of course renal disease • It is a useful guestimate of the Glomerular filtration rate (GFR).
Gentamicin Dosing - Infusion Gentamicin comes in 80mg vials. It is important to try and make your doses multiples of 40 to ease the nurses’ job in making up the infusion. Infusion 100ml 5% glucose or sodium chloride 0.9% over 60 minutes (round to the nearest 40mg) to a maximum of 400mg. Doses ≤ 240 mg – slow IV over 3 -5 minutes ≥ 240mg – over 30 minutes (as above) Note it can be given IM with good effect BUT be wary of DIC and raised INR in the sick or anticoagulated patient.
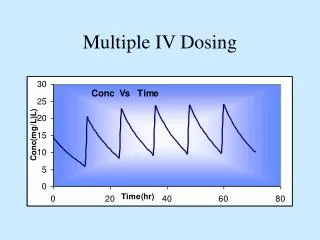
Monitoring of Levels After the initial BIG BOLUS • Take the ‘trough’ level 6 – 14 hours POST dose (conventionally 12 hours) • This trough level should be in the sub-therapeutic range. As shown on the graph <1 mg / l at 12hrs • This applies to all subsequent pre-dose levels. • If the trough or pre–dose level is still in the therapeutic window (between the black lines), the next dose should be missed or delayed.
Monitoring of Levels - II Pre level – (Trough) < 1mg/l Post level (Peak) > 8 mg/l • The post dose level is taken a minimum 30 minutes after dose – usually measured 1 hour post dose. • You don’t want it to be toooo high as this will mean that much of the dose is above the therapeutic range and therefore will cause toxicity. Frequency of levels • Ill patient – monitor daily or once / three days; Trough (Pre) level is important as are massive peaks. • Stable patient – STOP Treatment? Further levels once every three days • Multiple dosing (BD and TDS) – take levels after second (bd) or third (tds) dose; then rules above apply.
Gentamicin challenge You are the FY1 doctor on acute medical on-call. The next patient Mrs DB (DOB 18.12.46) is a previously fit and well woman who presents to A&E with a 24 hour history of delirium and offensive urine. She is haemodynamically stable. Your SpR has asked you to give her a stat dose of gentamicin and then write up her up for a course of IV cefuroxime. U&Es: Na+ 142; K+4.9; Urea 11.6; Cr 120 Her weight is guestimated at 80Kg • Calculate her creatinine clearance • How does this affect your dosing of her gentamicin? • Using the drug chart provided write up the gentamicin and course of IV cefuroxime. • What other therapeutic interventions will you write up?
Gentamicin challenge - Answers (1)Creatinine clearance (ml/min) = (N - age (years) ) x Wt (kg)serum creatinine (µmol/l) = (150 – 60) x 80 = 60ml/min 120 Please note – her age will increase by 1 year for each year this module is up and running! Change the calculation and answer accordingly. (2) This is a significantly reduced creatinine clearance and thus this patient should receive a maximum of 1-2 mg /kg i.e. maximum dose 160mg (3) See the chart on the next slide … (4) She should also be written up for IV fluids, anti-emetics and any regular medications.
So that’s what a slightly out of focus drug chart looks like!
Anticoagulation The verbs to Heparinise and to Warfarinise
Challenging Practice • Remember neither Heparin nor Warfarin ‘thin’ the blood. They both stop the blood clotting! • List three indications for heparin • List three side effects of heparin • Why may you use IV unfractionated heparin rather than SC low molecular weight heparin? • Which drug is used to reverse the anticoagulant effects of heparin?
Heparin • Naturally occurring glycosaminoglycan • Discovered in 1916 at John Hopkins University but was not used clinically in humans until the 1930s. • Derived from liver cells (‘Hepar’ is the Greek for ‘Liver’) • Two forms Unfractionated heparin (UH) and fractionated, low molecular weight heparin (LMWH) • May be given subcutaneously or intravenously • Should NEVER be given IM (think about it!)
Unfractionated Heparin (UH) • Given intravenously • Advantages - Rapidly reversed by turning off the infusion (typically half life is 30minutes, so APTT will return to normal within this period) - This it is still used in patients where they may be at risk of bleeding but still need anticoagulation; other indications include surgical patients, renal failure patients and cardiac catheter patients • Disadvantages - Binds unpredictably and non-specifically to plasma proteins, macrophages and vascular endothelium leading to an unpredictable response to dosing. - Binding to plasma proteins can lead to heparin resistance, where very large doses are required to achieve anticoagulation. • Side effects - Bleeding – if clinically significant needs to be reversed by (a) stopping the heparin and (b) giving IV protamine infusion or FFP - Heparin Induced Thrombocytopaenia [HIT] – heparin binds to platelet factor 4 forming a complex. UH may induce the production of an auto-antibody against this complex, which in turn causes thrombocytopaenia. Paradoxically (despite low platelets) there is an extension of existing thrombus and risk of further thrombosis. - Osteopaenia – UH binds to osteoblasts, activating osteoclasts and thus leasds to osteopaenia. This is only of concern in patients who need long term heparin e.g. pregnant women who have had a DVT or PE early in their pregnancy (Warfarin is contraindicated)
Unfractionated Heparin (UH) Dose (IV) • Load with 4000 - 5000units stat (IV) • Typically patients are then given between 20,000 and 50,000 units over 24hours (depending principally on their lean and total body weight) • Therapeutic level – aim to keep APTT at (2 – 3 x control - approx 60 – 90 seconds) • Monitor therapy by performing APTT at steady state (6 hours after the infusion begins) • Dose and infusion should then be adjusted accordingly (see http://www.hscj.ufl.edu/resman/manualpdfs/Heparin_Orders_Med_Surg_Crit_Care.pdf) • APTT needs to be checked at least once every 24hours after therapeutic level is achieved.
A quick calculation …http://www.hscj.ufl.edu/resman/manualpdfs/Heparin_Orders_Med_Surg_Crit_Care.pdf Mr James Watt is a 43yo man (d.o.b 12/04/63) (hospital number 203864) who is to be admitted from A&E with a suspected pulmonary embolism. He is ‘guestimated’ to be 80Kg. He has no known drug allergies. Using the link (above) and the IV heparin protocol provided • Write up the recommended heparin infusion on a fluid chart. • Please work out the rate of the infusion in units/hour and ml/hour. • At 6hours his APTT is 124seconds. Please recalculate the infusion rate in units/hr and ml/hr.
Mr Watt – The answers According to the protocol • Write up an infusion of 25,000units of heparin in 250ml 5% dextrose (D5W) i.e. 100units/ml; Mr Watt is 80kg • He should have had a stat dose of 5000u heparin IV (which would have been written on the drug chart once only section) • The infusion rate for a patient with a PE should run at 15units/kg/hr = (15x80)u/hr = 1200u/hr • If 100u/ml, this means the initial infusion rate is 12ml/hr. • If the APTT is 124 seconds – the protocol recommends that the infusion be turned off for 1 hour and then re-started at a rate of 3u/kg/hr less than before i.e. 12u/kg/hr • Thus new infusion rate = (12 x 80)u/hr = 960u/hr = 9.6ml/hr • See next slide for fluid chart
Fractionated LMWH • Derived by ‘fractionation’ or depolymerisation of the larger and longer chained, naturally occurring unfractionated heparin • Thus they are smaller molecules with shorter polysaccharide side chains • Principally work by blocking coagulation factor Xa (unlike UH which also blocks the action of thrombin) • They have less affinity to plasma proteins, macrophages, endothelium and osteoblasts • These features mean they: - cause less of the side effects of UH e.g. H.I.T and osteoporosis • are more predictable in effect. • have a longer half life and therefore need only be given once or twice / 24 hours • can be administered subcutaneously • Disadvantage – the long half life means they are less easily reversed so are not used in ‘high risk’ patients or those with need for rapid, simple reversal of their anticoagulation e.g. prior to operative intervention. • Side effects – Bleeding; Other side effects are similar to UH but at a far lower incidence . • However they can NOT be used as a substitute for UH in patients with H.I.T; In this case the heparinoid = Danaparoid is used. [Not to be confused with the antipsychotic Danisparanoid]
LMWH – Indications and Doses Indications – ACS, DVT and PE treatment and prophylaxis i.e. similar to those of UH but LMWHs are now are used as the heparins of choice. • Two LMWH are commonly used in the UK Enoxaparin (Clexane) and Dalteparin (Fragmin); Both are given subcutaneously • Both are dosed by units or mg / kg (thus you need to know or guestimate the patient’s weight) • Most hospitals will produce dose/Kg protocols for all their main indications
When to stop the Heparin • If the patient is on prophylaxis for DVT/PE the heparin may be stopped once they are mobilising well and clinically improving. • In patients with ACS – the heparin is stopped when they are pain free and mobilising well. • In orthopaedic patients who have undergone total hip replacement there is evidence to suggest that they should stay on heparin for several months post-operatively (although this is still not common practise). • For medical patients you should think whether the patient would benefit from long term anticoagulation with warfarin e.g. patients with AF. • In patients starting warfarin for DVT or PE, warfarin is started as soon as the diagnosis is confirmed. The heparin is then continued until the patient’s INR > 2.0. • However there is evidence that patients should stay on the heparin for several days from the time of their admission or diagnosis. This varies from 5 to 10 days (and is additional to the initiation of warfarin) – this is not common practise in the UK. • DVT therapy is now commonly initiated as an outpatient (from the A&E department) BUT all patients should be followed up to consider possible underlying causes.
Heparin Links • http://www.mja.com.au/public/issues/177_07_071002/eik10205_fm.html Nice summary of LMWH treatment • http://www.rxkinetics.com/heparin.html Nice summary of UH treatment (a little technified at the end!) • http://www.bcshguidelines.com/pdf/heparin_220506.pdf British Society for Haematology guidelines for heparin therapy – hot off the press 2006 • http://www.hscj.ufl.edu/resman/manualpdfs/Heparin_Orders_Med_Surg_Crit_Care.pdf
coumARIN anticoagulant + = WARFARIN
Challenging Practice • List three indications for Warfarin therapy • Write up a loading regime for a 41yo woman who is on subcutaneous heparin and has just had a left lower limb DVT confirmed • List the essential steps before discharging a patient on Warfarin • A 71yo man who is on long term warfarin treatment presents in A&E with a ‘torrential’ epistaxis. He is haemodynamically stable but his INR is 9.9. What is your management?
Warfarin • The most famous coumarin anticoagulant (name another!) • Developed at The Wisconsin Alumni Research Foundation ( http://www.warf.ws/- for the non-believers!) • Hence its name WARFarin • Indications - Venous thrombo –embolic disease - Pulmonary embolism - Arterial thrombosis - Atrial fibrillation / Stroke prophylaxis (primary and secondary) - Prosthetic heart valve - Left ventricular aneurysm and large intra-cardiac thrombus (primarily seen post MI) • Main side effect – Increased risk of bleeding • Famously causes idiosyncratic skin necrosis at large doses see … (http://pathology.uc.edu/LABLINES/V7I6.pdf ) Warfarin induced skin necrosis
Monitor INR • Therapeutic levels based on INR • Target INR 2 – 3: DVT, PE, AF, Arterial thrombosis INR 3 – 4: Metallic heart valve • Warfarin levels will not reach steady state for several days so early INRs may be misleading
Fennerty nomogramFennerty A, Thomas P, Backhouse G, Bentley DP, Campbell IA, Routledge PA. Flexible induction dose regimen for warfarin and prediction of maintenance dose. Br Med J 1984; 288:1268-70. This protocol was designed to • achieve a target INR of 2 to 3 relatively quickly. • reduce the risk of overanticoagulation which is more likely to occur in patients who exhibit greater sensitivity to warfarin (eg elderly patients, patients with liver disease, inadequate nutrition, or CHF). • However: it does not eliminate INR overswings entirely, and a lower loading dose of 5mg may be used in patients thought to be especially at risk. • It now appears in a modified form in the specific anticoagulation part of many Trust drug charts (I.e. you don’t have to memorise it!)
Warfarin Dosing - II Day INR Warfarin dose (mg) Predicted maintenance dose: 4th Day 1st < 1.4 10 INR Warfarin (mg) 2nd < 1.8 10 <1.4 >8 1.8 1.0 1.4 8 > 1.8 0.5 1.5 7.5 3rd <2.0 10 1.6-1.7 7 2.0-2.1 5 1.8 6.5 2.2-2.3 4.5 1.9 6 2.4-2.5 4 2.0-2.1 5.5 2.6-2.7 3.5 2.2-2.3 5 2.8-2.9 3 2.4-2.6 4.5 3.0-3.1 2.5 2.7-3.0 4 3.2-3.3 2 3.1-3.5 3.5 3.4 1.5 3.6-4.0 3 3.5 1.0 4.1-4.5 Miss out next day's 3.6-4.0 0.5 dose, then give 2mg >4.0 0 >4.5 Miss out 2 days' doses then give 1mg
Warfarin and Haemorrhage • Haemorrhage is the principal side effect of warfarin therapy • The risk is said to increase exponentially once INR goes above 5.0 – particularly spontaneous intra-cranial haemorrhage • However 50% of patients who have bleeds whilst on warfarin have INR< 4.0 • The risk of haemorrhage is increased by: - Increasing age > 65yo (although this is multifactorial and may be related more to increased co-morbidities and polypharmacy) - Co-morbidities – liver disease, hypertension, renal failure, thrombocytopaenia and coagulopathy - Drugs – enzyme inhibitors, alcohol excess, NSAIDs - Previous GI or other significant haemorrhage.
Bleeding Hell! – What to do about it • Major bleeding—stop warfarin; give vitamin K1 - 5 mg by slow intravenous injection; give prothrombin complex concentrate PCC (factors II, VII, IX and X) 50 units/kg or (if no concentrate available) fresh frozen plasma 15 m/kg • INR > 8.0, no bleeding or minor bleeding—stop warfarin, restart when INR < 5.0; if there are other risk factors for bleeding give vitamin K1 0.5 mg by slow intravenous injection or 5 mg by mouth (for partial reversal of anticoagulation give smaller oral doses of vitamin K e.g. 0.5–2.5 mg using the intravenous preparation orally); repeat dose of vitamin K if INR still too high after 24 hours • INR 6.0–8.0, no bleeding or minor bleeding—stop warfarin, restart when INR < 5.0 • INR < 6.0 but more than 0.5 units above target value—reduce dose or stop warfarin, restart when INR < 5.0 • Unexpected bleeding at therapeutic levels—always investigate possibility of underlying cause e.g. unsuspected renal or gastro-intestinal tract pathology British Society for Haematology Guidelines as per BNF 2003
For the Warfarin addicted …. http://www.acforum.org/doc_education_management.ppt#316 Another very nice overview of warfarin therapy – with really pretty slides! A little out of date in parts but very good on the basic science. http://www.bcshguidelines.com/pdf/oralanticoagulation.pdf British Society for Haematology guidelines (2005) on oral anticoagulation – everything you want to know and more! http://www.mja.com.au/public/issues/181_09_011104/bak10441_fm.html#CHDDCIFC Another excellent overview from our friends down under – good on ya!
Be warned! • All patients placed on warfarin should be booked into a specialist anticoagulation clinic before being discharged. • They should receive an anticoagulation booklet once established on warfarin • Because it is a commonly prescribed drug which has potentially serious side effects, multiple interactions and ‘complex’ follow up, warfarin is the beloved drug of exams and examiners in the latter phase of the course • Lots of OSCE potential there!
Challenging Practice • List two indications for digoxin • List three biochemical abnormalities which will potentiate digoxin toxicity. • List the common ECG changes seen with digoxin. • What is the name of the drug used in severe digoxin toxicity?
Digoxin • Digoxin is a cardiac glycoside derived from the Foxglove plant – ‘Digitalis purpurea’ • Has been used by native tribesmen for centuries as a toxin for their darts and arrows • First used for cardiac conditions by the Romans • Famously described by William Withering in 1785 as a treatment for ‘Dropsy’ (oedema) • Indications – Supraventricular tachyarrythmia (AF, Aflutter) – More recently its use is being superseded by betablockers, rate limiting calcium channel blockers, as well as amiodarone. - Heart failure – likewise, its use has become restricted to end stage disease • Caution – Reduced Creatinine clearance (see gentamicin section); Hypokalaemia • Toxic effects potentiated by Hypokalaemia, hypomagnesaemia (both commonly caused by diuretic therapy) and hypercalcaemia. Both hypomagnesaemia and hypercalcaemia interfere with its effect on Na+/K+ ATPase.
Digoxin Dosing • Loading (PO or IV) - Patient needs ECG monitoring - Loading dose 250 – 500 mcg (depending on creatinine clearance) - Further similar, repeat dose is given 8 hours later - Maintenance dose at 24 hours (from first loading dose) = 62.5 – 125 mcg - If rate is still poorly controlled dose can be increased in 62.5mcg increments to a maximum of 250 mcg / day
Side effects and interactions Side effects • Arrhythmia (classically bradycardia and various degrees of heart block. Allegedly digoxin toxicity may cause any tachy or bradyarrhythmia!) • Nausea and vomiting, diarrhoea. ‘Slow (bradycardia) and Sick’ – Digoxin toxicity ‘Fast (tachycardia) and Sick’ – Aminophylline toxicity • Dizziness and confusion. • Famously –Xanthopsia – Yellow (and green) colouring of the vision • In practice – most patients (including the elderly!) have no problems on digoxin (Despite its NTW and their co-morbidities) Interactions • Bradycardia inducing agents – betablockers, rate limiting calcium channel blockers, amiodarone • Quinidine • Erythromycin
Monitoring therapy • Levels are taken on day (7 or after) of therapy as this is when steady state is reached. Levels taken before this can often be misleading. • The level is taken at least 6 hours after the last dose (this may also be a cause of false concern when levels performed on admission fall well within this 6 hour cut-off.) • However very low or non-existent concentrations on admission may confirm the diagnosis of poor compliance. • Normal range 1.0 – 2.6 nmol/l • This may vary according to different labs • Toxicity may occur within the normal range when other factors e.g. hypokalaemia exist.
Digoxin Toxicity • Toxicity often presents with non-specific signs and symptoms and as with any patient on medications one needs a very high index of suspicion! • Remember - Drugs cause everything! - ‘Slow and Sick’ – Digoxin toxicity - The ‘reverse tick sign on an ECG is a sign of digoxin therapy and not toxicity! - Regular VEBs, Bradycardia, heart block and arrhythmia may all be signs of digoxin toxicity • Correct hypokalaemia and other biochemical abnormalities • Correct treatable causes of renal impairment • For Severe Toxicity / Overdose one can give (Digibind ®) an IV preparation made of Digoxin-specific antibody fragments.
DIGOXIN Challenge A 78yo man with COPD presents in A&E with a right lower lobe pneumonia and fast AF. U+Es:Na+ 141mmol/l, K+ 4.1 mmol/l Urea 32.8 mmol/l, Creatinine 140µmol/l. He is guestimated to weigh 60kg. He has no known allergies. The lovely 3rd year medical student has written up the patient’s details for you. • Calculate his creatinine clearance • Write up the loading and maintenance doses of digoxin on your charts. You should also write up the other medications you would give him. • List three other investigations he may require.
Digoxin challenge - Answers (1) Creatinine clearance (ml/min) = (N - age (years) ) x Wt (kg) serum creatinine (µmol/l) = (160 – 78) x 60 = 35.1ml/min 140 (2) See charts on the next 3 slides for answers (3) FBC, Repeat U+Es, Calcium and magnesium, Blood and sputum cultures Chest radiograph ECG ABGs When heart rate is improved - Echocardiogram