Download
1 / 1
10 likes | 198 Views
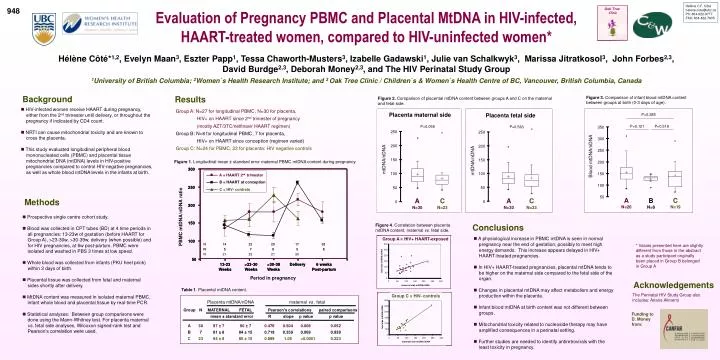
Oak Tree Clinic. Placenta maternal side. Placenta fetal side. P=0.058. P=0.563. 250. 250. 300. 300. A = HAART 2. A= HAART 2. trimester. trimester. nd. nd. 200. 200. B= HAART conception. B = HAART at conception. 250. 250. mtDNA/nDNA. C = HIV. C= HIV. -. -. controls.

E N D
Oak Tree Clinic Placenta maternal side Placenta fetal side P=0.058 P=0.563 250 250 300 300 A = HAART 2 A= HAART 2 trimester trimester nd nd 200 200 B= HAART conception B = HAART at conception 250 250 mtDNA/nDNA C = HIV C= HIV - - controls controls mtDNA/nDNA 150 150 ratio 100 200 200 nDNA 100 50 50 150 150 PBMC mtDNA/ A N=30 C N=23 A N=30 C N=23 0 0 100 100 50 50 13 13 - - 23 23 >23 >23 - - 30 30 >30 >30 - - 39 39 Delivery Delivery 6 weeks 6 weeks Weeks Weeks Weeks Weeks Weeks Weeks Post Post - - partum partum N 14 22 28 17 28 Period in pregnancy N 5 7 8 5 8 N 21 22 21 20 Placenta mtDNA/nDNA maternal vs . fetal Group N MATERNAL FETAL Pearson's correlations paired comparisons mean ± standard error R slope p value p value A 30 97 ± 7 90 ± 7 0.476 0.504 0.008 0.052 B 7 81 ± 8 84 ± 15 0.719 0.359 0.069 0.938 C 23 84 ± 8 85 ± 10 0.899 1.05 <0.0001 0.223 Hélène C.F. Côté helene.cote@ubc.ca Ph: 604-822-9777 FAX: 604-822-7635 948 Evaluation of Pregnancy PBMC and Placental MtDNA in HIV-infected, HAART-treated women, compared to HIV-uninfected women* Hélène Côté*1,2, Evelyn Maan3, Eszter Papp1, Tessa Chaworth-Musters3, Izabelle Gadawski1, Julie van Schalkwyk3, Marissa Jitratkosol3, John Forbes2,3, David Burdge2,3, Deborah Money2,3, and The HIV Perinatal Study Group 1University of British Columbia; 2Women`s Health Research Institute; and 3 Oak Tree Clinic / Children`s & Women`s Health Centre of BC, Vancouver, British Columbia, Canada Background Results Figure 3. Comparison of infant blood mtDNA content between groups at birth (0-3 days of age). Figure 2. Comparison of placental mtDNA content between groups A and C on the maternal and fetal side. • HIV-infected women receive HAART during pregnancy, either from the 2nd trimester until delivery, or throughout the pregnancy if indicated by CD4 count. • NRTI can cause mitochondrial toxicity and are known to cross the placenta. • This study evaluated longitudinal peripheral blood mononucleated cells (PBMC) and placental tissue mitochondrial DNA (mtDNA) levels in HIV-positive pregnancies compared to control HIV-negative pregnancies, as well as whole blood mtDNA levels in the infants at birth. Group A: N=27 for longitudinal PBMC, N=30 for placenta, HIV+ on HAART since 2nd trimester of pregnancy (mostly AZT/3TC/nelfinavir HAART regimen) Group B: N=8 for longitudinal PBMC, 7 for placenta, HIV+ on HAART since conception (regimen varied) Group C: N=24 for PBMC, 23 for placenta: HIV negative controls P=0.285 P=0.121 P=0.518 350 300 250 Blood mtDNA/nDNA Figure 1. Longitudinal mean ± standard error maternal PBMC mtDNA content during pregnancy. 200 150 100 50 Methods A N=26 C N=19 B N=8 • Prospective single centre cohort study. • Blood was collected in CPT tubes (BD) at 4 time periods in all pregnancies: 13-23w of gestation (before HAART for Group A), >23-30w, >30-39w, delivery (when possible) and for HIV pregnancies, at 6w post-partum. PBMC were isolated and washed in PBS 3 times at low speed. • Whole blood was collected from infants (PKU heel prick) within 3 days of birth. • Placental tissue was collected from fetal and maternal sides shortly after delivery. • MtDNA content was measured in isolated maternal PBMC, infant whole blood and placental tissue by real-time PCR. • Statistical analyses: Between group comparisons were done using the Mann-Whitney test. For placenta maternal vs. fetal side analyses, Wilcoxon signed-rank test and Pearson’s correlation were used. Conclusions Figure 4. Correlation between placenta mtDNA content, maternal vs. fetal side. • A physiological increase in PBMC mtDNA is seen in normal pregnancy near the end of gestation, possibly to meet high energy demands. This increase appears delayed in HIV+ HAART-treated pregnancies. • In HIV+ HAART-treated pregnancies, placental mtDNA tends to be higher on the maternal side compared to the fetal side of the organ. • Changes in placental mtDNA may affect metabolism and energy production within the placenta. • Infant blood mtDNA at birth content was not different between groups. • Mitochondrial toxicity related to nucleoside therapy may have amplified consequences in a perinatal setting. • Further studies are needed to identify antiretrovirals with the least toxicity in pregnancy. Group A = HIV+ HAART-exposed * Values presented here are slightly different from those in the abstract as a study participant originally been placed in Group B belonged in Group A 300 250 200 fetal side mtDNA/nDNA 150 100 50 0 Acknowledgements 0 50 100 150 200 250 300 maternal side mtDNA/nDNA Table 1. Placental mtDNA content. The Perinatal HIV Study Group also includes: Ariane Alimenti Group C = HIV- controls 300 250 200 Funding to D. Money from: fetal side mtDNA/nDNA 150 100 50 0 0 50 100 150 200 250 300 maternal side mtDNA/nDNA