Download
1 / 30
300 likes | 470 Views
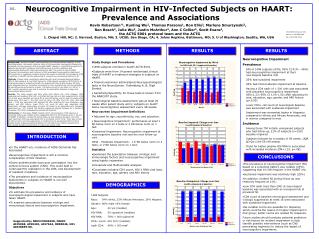
Outcomes of HAART in HIV infected individuals in Argentina. Carlos Zala, Robert Hogg, Horacio Salomon, Keith Chan, Mariana Ceriotto, Marcelo Beltran, Miriam Burgos, Pedro Cahn, JSG Montaner and the PUMA study group Buenos Aires, Argentina

E N D
Outcomes of HAART in HIV infected individuals in Argentina Carlos Zala, Robert Hogg, Horacio Salomon, Keith Chan, Mariana Ceriotto, Marcelo Beltran, Miriam Burgos, Pedro Cahn, JSG Montaner and the PUMA study group Buenos Aires, Argentina BC Center for Excellence in HIV/AIDS. Vancouver, BC. Canada PUMA
2.5 Millions 2.0 1.5 Number of people living with HIV 1.0 0.5 0.0 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 Year AIDS epidemic update, December 2005 Latin America and Caribbean Number of people living with HIV in Latin America and Caribbean, 1986–2005
Background • The Argentinean government has made a commitment to provide free HAART to eligible individuals (IAS-USA guidelines) • Limited data are available on subjects who initiates HAART in Argentina PUMA
Potential limitations of HAART use in Argentina • Use of generic ARVs • Limited or restricted use of newer drugs • Endemic OIs • High TB prevalence • Lack of drug resistant testing • Physicians have variable experience with HAART • Heterogeneous sources of HIV care PUMA
Prospective evaluation in the Use and Monitoring of Antiretrovirals in Argentina:The PUMA Cohort Ongoing multi-site based cohort at HIV clinics throughout Argentina PUMA
Objective (1) • To evaluate baseline plasma HIV RNA, CD4 T cell counts among ARV naïve HIV positive subjects initiating HAART at selected public hospitals PUMA
Objective (2) • To describe AIDS related morbidity and mortality, changes in plasma HIV RNA and CD4 T cell counts among patients who initiated HAART PUMA
Eligibility Criteria • All consecutive ARV naïve HIV infected individuals seeking treatment or care • Age 18 or older • Known data of initiation of HAART • HIV RNA and CD4 within 3 mo from BSL • CDC clinical stage (pre-HAART) PUMA
Treatment, labs and follow-up • HAART: any boosted-PI or NNRTI + 2 NRTI • Free access to routine lab monitoring • Lost to follow-up: missing laboratory values > 6 months • AIDS related death (CDC) PUMA
Data collection • Prospective/ standardized data collection at 10 sites • Data entry at a single Coordinating Center • Anonymous data pooled for analysis • IRB approval PUMA
Types of data collected • Sociodemographic data • HAART treatment history • Laboratory tests, including CD4 and HIV RNA • Reasons for interruption, switching and failure • AIDS defining illnesses/ death PUMA
Results • 605 participants enrolled from Jan 03 to Dec 05 • 299 (49%) initiated HAART upon entering the program • 93 (36%) initiated HAART during follow-up • Median follow-up 17.8 months (IQR: 6.6-26.4) • 85 (14 %) lost to follow up
Results • 605 participants enrolled from Jan 03 to Dec 05 • 299 (49%) initiated HAART upon entering the program • 93 (36%) initiated HAART during follow-up • Median follow-up 17.8 months (IQR: 6.6-26.4) • 85 (14 %) lost to follow up
PUMA: Baseline (n = 605) * Median (interquartile range); (+) according ot CDC 1987 case definition
Baseline HAART * Wilcoxon Rank Sum Test ** median (interquartile range)
Time to start of HAART * at baseline
Most common OIs at entry * (includes presumptive and confirmed cases)
Most common initial regimen (%) * LVP/r, Atazanavir/r; ** Generic of Combivir
Reasons for switching first HAART regimen • 96/387 (25%) • Gastrointestinal (25%) • Intolerance (21%) • Anemia (11 %) • Skin reactions (8.5 %) • Physician indication (8.5 %) • Virologic failure (3.5 %) • CNS (1.7 %)
Plasma HIV RNA and CD4 changes from baseline % HIV RNA n=272 n=272
AIDS related deaths (n=15) • Histoplasmosis 1 • LNH 3 • TB 1 • Toxoplasmosis 1 • SK 1 • Cryptococosis 2 • SK 1 • LMP 1 • ESLD 2 • UNK 2
Limitations • Lack of active follow-up procedures • No tracking lost to follow up patients • Death reported only if occurred at the participating institutions • Evaluation of Adherence PUMA
Conclusions • First prospective HAART cohort in Argentina • Initiation of HAART was associated with advanced HIV disease • Proportion of patients with early virologic response similar to that reported in other cohorts • Urgent efforts are needed to optimize timing of initiation of HAART in this setting PUMA
The PUMA study group - Argentina Acknowledgments Hospital de Jujuy (Carlos Ramondegui) CNRS (Horacio Salomon) Hospital Paroissien (Eduardo Warley) Hospital Fernandez (Carlos Zala/Pedro Cahn) • Center for Excellence in HIV/aids – Vancouver, BC. Canada Robert Hogg Keith Chan Nada Gataric Julio SG Montaner Hospital de San Isidro (Marcelo Beltran) Hospital Tornu (Miriam Burgos/Viviana Rodriguez) Hospital Alberdi (Raul Bortolozi) Hospital de Neuquen (Liliana Calani) Helios Salud (Isabel Cassetti) Hospital Cecilia Grierson (Mariana Ceriotto) Hospital San Juan de Dios (Jorge Contarelli) Hospital de Mar del Plata (Alejandro Ferro) Hospital Misericordia (Angel Minguez) Hospital de San Fernando (Fernando Murano) Funcei (Gustavo Lopardo) Hospital Velez Sarfield (Daniel Pryluka) PUMA
Statistics • Categorical variables were compared between groups using Pearson’s chi-squared test and Fisher’s exact test. • Comparisons of continuous variables were carried out using Wilcoxon’s rank-sum test. • Kaplan Meier methods and Cox proportional hazard regression were used to analyze time to event outcomes. PUMA
Quarterly accrual 2003-2005 2003 2005 2004