Download
1 / 1
40 likes | 280 Views
Malignant Melanoma of the Nasal Cavity- Case report 鼻腔內惡性黑色素瘤 - 病例報告. 1 張聰舜 2 王興萬 1 三軍總醫院耳鼻喉頭頸外科部 2 雙和醫院耳鼻喉科 1 Tsung-Shun Chang, 2 Hsing-Won Wang 1 Department of Otolaryngology-Head and Neck Surgery, Tri-Service General Hospital

E N D
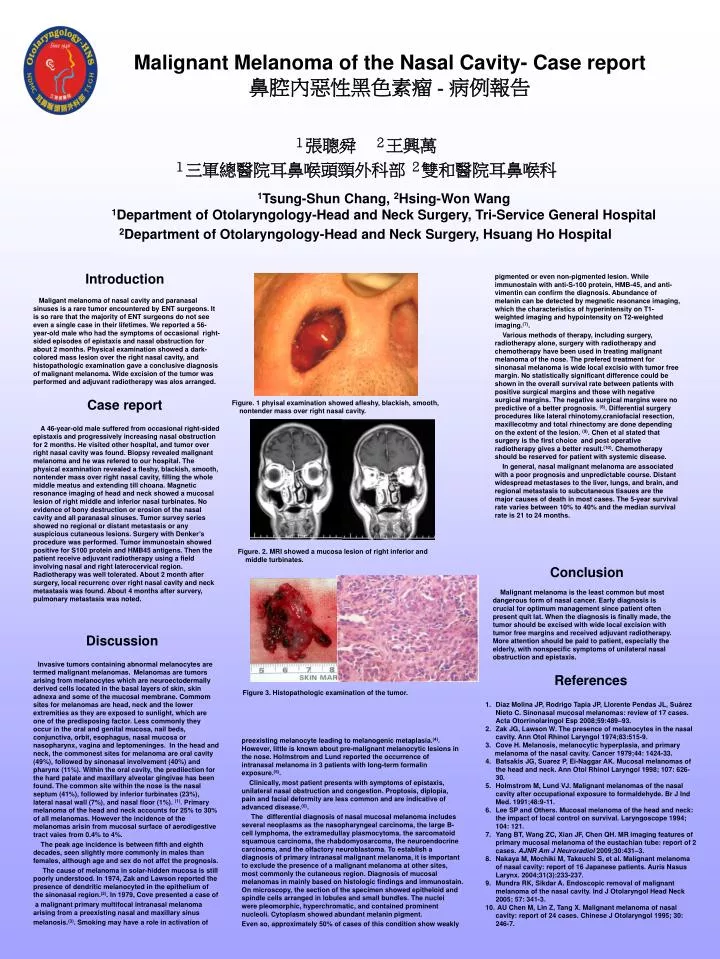
Malignant Melanoma of the Nasal Cavity- Case report鼻腔內惡性黑色素瘤 - 病例報告 1張聰舜 2王興萬 1三軍總醫院耳鼻喉頭頸外科部2雙和醫院耳鼻喉科 1Tsung-Shun Chang, 2Hsing-Won Wang 1Department of Otolaryngology-Head and Neck Surgery,Tri-Service General Hospital 2Department of Otolaryngology-Head and Neck Surgery, Hsuang Ho Hospital pigmented or even non-pigmented lesion. While immunostain with anti-S-100 protein, HMB-45, and anti-vimentin can confirm the diagnosis. Abundance of melanin can be detected by megnetic resonance imaging, which the characteristics of hyperintensity on T1-weighted imaging and hypointensity on T2-weighted imaging.(7). Various methods of therapy, including surgery, radiotherapy alone, surgery with radiotherapy and chemotherapy have been used in treating malignant melanoma of the nose. The prefered treatment for sinonasal melanoma is wide local excisio with tumor free margin. No statistically significant difference could be shown in the overall survival rate between patients with positive surgical margins and those with negative surgical margins. The negative surgical margins were no predictive of a better prognosis. (8). Differential surgery procedures like lateral rhinotomy,craniofacial resection, maxillecotmy and total rhinectomy are done depending on the extent of the lesion. (9). Chen et al stated that surgery is the first choice and post operative radiotherapy gives a better result.(10). Chemotherapy should be reserved for patient with systemic disease. In general, nasal malignant melanoma are associated with a poor prognosis and unpredictable course. Distant widespread metastases to the liver, lungs, and brain, and regional metastasis to subcutaneous tissues are the major causes of death in most cases. The 5-year survival rate varies between 10% to 40% and the median survival rate is 21 to 24 months. Introduction Maligant melanoma of nasal cavity and paranasal sinuses is a rare tumor encountered by ENT surgeons. It is so rare that the majority of ENT surgeons do not see even a single case in their lifetimes. We reported a 56-year-old male who had the symptoms of occasional right-sided episodes of epistaxis and nasal obstruction for about 2 months. Physical examination showed a dark-colored mass lesion over the right nasal cavity, and histopathologic examination gave a conclusive diagnosis of malignant melanoma. Wide excision of the tumor was performed and adjuvant radiotherapy was alos arranged. Case report Figure. 1 phyisal examination showed afleshy, blackish, smooth, nontender mass over right nasal cavity. A 46-year-old male suffered from occasional right-sided epistaxis and progressively increasing nasal obstruction for 2 months. He visited other hospital, and tumor over right nasal cavity was found. Biopsy revealed malignant melanoma and he was refered to our hospital. The physical examination revealed a fleshy, blackish, smooth, nontender mass over right nasal cavity, filling the whole middle meatus and extending till choana. Magnetic resonance imaging of head and neck showed a mucosal lesion of right middle and inferior nasal turbinates. No evidence of bony destruction or erosion of the nasal cavity and all paranasal sinuses. Tumor survey series showed no regional or distant metastasis or any suspicious cutaneous lesions. Surgery with Denker’s procedure was performed. Tumor immunostain showed positive for S100 protein and HMB45 antigens. Then the patient receive adjuvant radiotherapy using a field involving nasal and right laterocervical region. Radiotherapy was well tolerated. About 2 month after surgery, local recurrenc over right nasal cavity and neck metastasis was found. About 4 months after survery, pulmonary metastasis was noted. Figure. 2. MRI showed a mucosa lesion of right inferior and middle turbinates. Conclusion Malignant melanoma is the least common but most dangerous form of nasal cancer. Early diagnosis is crucial for optimum management since patient often present quit lat. When the diagnosis is finally made, the tumor should be excised with wide local excision with tumor free margins and received adjuvant radiotherapy. More attention should be paid to patient, especially the elderly, with nonspecific symptoms of unilateral nasal obstruction and epistaxis. Discussion Invasive tumors containing abnormal melanocytes are termed malignant melanomas.Melanomas are tumors arising from melanocytes which are neuroectodermally derived cells located in the basal layers of skin, skin adnexa and some of the mucosal membrane. Commom sites for melanomas are head, neck and the lower extremities as they are exposed to sunlight, which are one of the predisposing factor. Less commonly they occur in the oral and genital mucosa, nail beds, conjunctiva, orbit, esophagus, nasal mucosa or nasopharynx, vagina and leptomeninges. In the head and neck, the commonest sites for melanoma are oral cavity (49%), followed by sinonasal involvement (40%) and pharynx (11%). Within the oral cavity, the predilection for the hard palate and maxillary alveolar gingivae has been found. The common site within the nose is the nasal septum (41%), followed by inferior turbinates (23%), lateral nasal wall (7%), and nasal floor (1%). (1). Primary melanoma of the head and neck accounts for 25% to 30% of all melanomas. However the incidence of the melanomas arisin from mucosal surface of aerodigestive tract vaies from 0.4% to 4%. The peak age incidence is between fifth and eighth decades, seen slightly more commonly in males than females, although age and sex do not affct the prognosis. The cause of melanoma in solar-hidden mucosa is still poorly understood. In 1974, Zak and Lawson reported the presence of dendritic melanocyted in the epithelium of the sinonasal region.(2). In 1979, Cove presented a case of a malignant primary multifocal intranasal melanoma arising from a preexisting nasal and maxillary sinus melanosis.(3). Smoking may have a role in activation of References Figure3. Histopathologic examination of the tumor. • Díaz Molina JP, Rodrigo Tapia JP, Llorente Pendas JL, Suárez Nieto C. Sinonasal mucosal melanomas: review of 17 cases. Acta Otorrinolaringol Esp 2008;59:489–93. • Zak JG, Lawson W. The presence of melanocytes in the nasal cavity. Ann Otol Rhinol Laryngol 1974;83:515-9. • Cove H. Melanosis, melanocytic hyperplasia, and primary • melanoma of the nasal cavity. Cancer 1979;44: 1424-33. • Batsakis JG, Suarez P, Ei-Naggar AK. Mucosal melanomas of the head and neck. Ann Otol Rhinol Laryngol 1998; 107: 626-30. • Holmstrom M, Lund VJ. Malignant melanomas of the nasal cavity after occupational exposure to formaldehyde. Br J Ind Med. 1991;48:9-11. • Lee SP and Others. Mucosal melanoma of the head and neck: the impact of local control on survival. Laryngoscope 1994; 104: 121. • Yang BT, Wang ZC, Xian JF, Chen QH. MR imaging features of primary mucosal melanoma of the eustachian tube: report of 2 cases. AJNR Am J Neuroradiol 2009;30:431–3. • Nakaya M, Mochiki M, Takeuchi S, et al. Malignant melanoma of nasal cavity: report of 16 Japanese patients. Auris Nasus Larynx. 2004;31(3):233-237. • Mundra RK, Sikdar A. Endoscopic removal of malignant melanoma of the nasal cavity. Ind J Otolaryngol Head Neck 2005; 57: 341-3. • AU Chen M, Lin Z, Tang X. Malignant melanoma of nasal cavity: report of 24 cases. Chinese J Otolaryngol 1995; 30: 246-7. preexisting melanocyte leading to melanogenic metaplasia.(4). However, little is known about pre-malignant melanocytic lesions in the nose. Holmstrom and Lund reported the occurrence of intranasal melanoma in 3 patients with long-term formalin exposure.(5). Clinically, most patient presents with symptoms of epistaxis, unilateral nasal obstruction and congestion. Proptosis, diplopia, pain and facial deformity are less common and are indicative of advanced disease.(6). The differential diagnosis of nasal mucosal melanoma includes several neoplasms as the nasopharyngeal carcinoma, the large B-cell lymphoma, the extramedullay plasmocytoma, the sarcomatoid squamous carcinoma, the rhabdomyosarcoma, the neuroendocrine carcinoma, and the olfactory neuroblastoma. To establish a diagnosis of primary intranasal malignant melanoma, it is important to exclude the presence of a malignant melanoma at other sites, most commonly the cutaneous region. Diagnosis of mucosal melanomas in mainly based on histologic findings and immunostain. On microscopy, the section of the specimen showed epitheloid and spindle cells arranged in lobules and small bundles. The nuclei were pleomorphic, hyperchromatic, and contained prominent nucleoli. Cytoplasm showed abundant melanin pigment. Even so, approximately 50% of cases of this condition show weakly