Download
1 / 99
1k likes | 1.2k Views
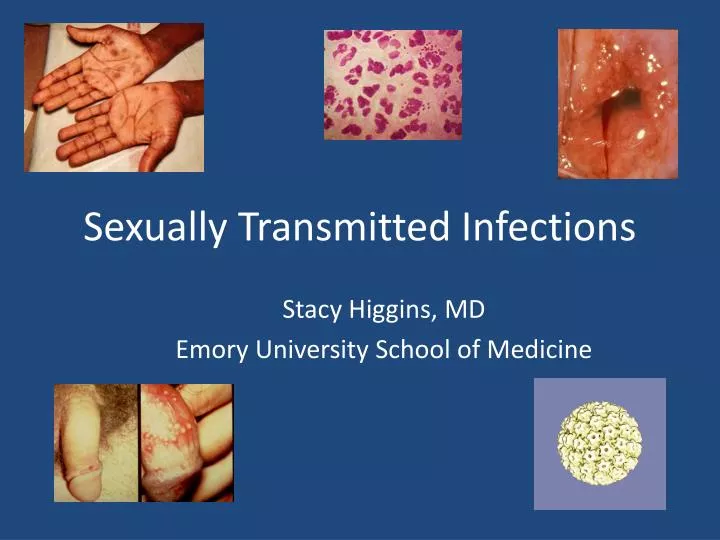
Sexually Transmitted Infections. Stacy Higgins, MD Emory University School of Medicine. Most Common STIs. Ulcerative Lesions Syphilis Genital Herpes Human Papilloma Virus Genital Warts Cervical Cancer Discharges Gonorrhea Chlamydia. History of Syphilis.

E N D
Sexually Transmitted Infections Stacy Higgins, MD Emory University School of Medicine
Most Common STIs • Ulcerative Lesions • Syphilis • Genital Herpes • Human Papilloma Virus • Genital Warts • Cervical Cancer • Discharges • Gonorrhea • Chlamydia
History of Syphilis • At the end of the 15th Century, syphilis arrived in Western Europe • “The French disease” or “The Disease of Naples” since the first cases had developed in that city during the French occupation • People believed to have suffered from syphilis
The Tuskegee Study • 1932: the USPHS enrolls 412 poor African American men diagnosed with syphilis in Macon County, Alabama • Goal: follow the natural course of the disease • Recruitment incentives: • Free medical care • Free hot meals • A certificate signed by the Surgeon General • $50 dollar burial stipend
Tuskegee Study • By 1943, penicillin was widely used to treat syphilis, except among the men in the Tuskegee study • The study stopped in 1972, when a CDC staff member blew the whistle
“He Who Knows Syphillis, Knows Medicine” Sir William Osler
Reported cases by stage of infection 1941–2005 Syphilis — Reported cases by stage of infection: United States, 1941–2005
Primary and secondary syphilis rates by state, 2005 The total rate of primary and secondary syphilis for the United States and outlying areas (Guam, P.R. and USVI) was 3 per 100,000. The Healthy People 2010 target is 0.2 case per 100,000 population.
Primary syphilis: CHANCRE • single, painless, clean based ulcer with induration • painless regional lymphadenopathy (80%) • incubation period of 3 to 90 days • occur at site of innoculation
Secondary Syphilis • 2w-6 mos after primary infection • Primary chancre may or may not still be present • Skin rash • Alopecia • Mucosal lesions • Generalized LAN
Syphilis- Latent stage • Latent Syphilis: period from disappearance of secondary symptoms until cure or tertiary symptoms • Early latent: within 1 year of infection • Late latent: after 1 year of infection
Tertiary Syphilis • Cardiovascular: • syphilitic aortitis of ascending aorta • aortic regurgitation • Neurologic: • asymptomatic • aseptic meningitis • paresis mimicking progressive dementia with psychotic features • tabes dorsalis
Epidemiology • Caused by HSV-1 or HSV-2 • Primary route of acquisition of HSV-2 is through genital-genital sexual contact • HSV-1 primarily acquired through oral-genital contact • Most cases subclinical • Transmission primarily from subclinical infection
Epidemiology • 25% of the US population over 30yo has HSV-2 • One of the 3 most common STDs • Genital Herpes: • HSV-2: 80-90%, • HSV-1: 10-20% • Risk of infection correlates with the number of lifetime sexual partners
Herpes: Initial Infection • “Classic” presentation: macules and papules that progress to vesicles, pustules and ulcers • Symptomatic cases sometimes severe with prolonged, systemic manifestations • Vesicles painful ulcerations crusting
Kimberlin and Rouse NEJM 350 (19): 1970, Figure 2 May 6, 2004
Herpes: Recurrent Infection • May be symptomatic or more commonly asymptomatic • Prodrome may be present • Duration of viral shedding is shorter and there are fewer lesions present • Recurrence rates decrease over time
Herpes and HIV • High HIV titers found in genital herpes ulcerations • Plasma HIV viral load increases with HSV-2 infection reactivation in HIV-infected persons
Underdiagnosis of Genital Herpes • 779 women attending STD clinic • 372 genital herpes diagnosis • Of the 372 diagnosed: • 82 (22%) symptomatic • 14 (4%) viral shedding without symptoms • 60 (14%) history of symptoms • 216 (58%) HSV-2 antibody without viral shedding or history of symptoms
HSV: Diagnosis • Tzanck smear • multinucleated giant cells ~2/3rds of the time when vesicles are present • often negative at the stage of crusting • Viral Culture • becomes insensitive within days of onset • Polymerase Chain Reaction • Type-specific serum antibody assays
Therapy- Initial Episode • Acyclovir 200mg 5x/day or 400mg TID x7-10d • Valacyclovir 1000mg BID x7-10d • Famciclovir 250mg TID x7-10d • Increased rate of healing, but does not prevent recurrences
HSV Recurrence • Recurrence seen in ~50% of people with symptomatic HSV within 6 months • Recurrence in ~80% by one year • Recurrence associated with stress, fever, menstruation, and intercourse
Episodic Recurrence Therapy • Acyclovir 400mg TID x5 days or 800mg TID x2 days • Valacyclovir 500mg BID for 3 days • Famciclovir 125mg BID x5 days • Only shortens duration if started within 24h
Suppressive Therapy • Acyclovir ($1500) or valacyclovir ($2500) or famciclovir ($2700) • Offered to those with >6 recurrences/year or severe outbreaks • Can reduce frequency of symptoms by 85% • Reduced frequency of subclinical viral shedding • Reduces risk of transmission of HSV to uninfected partners
Reducing Transmission • Recommend consistent condom use • Use of antiviral suppressive therapy to reduce viral shedding • Herpevac currently under study
Chlamydia • Nearly 1 million cases reported in 2005 • Infection caused by the intracellular parasite Chlamydia trachomatis • Asymptomatic infection with serious sequelae
Chlamydia — Rates: total and by sex United States, 1986–2005
Chlamydia — Rates by region United States, 1996–2005
Chlamydia — Rates by state United States and outlying areas, 2005
Chlamydia — Rates by race/ethnicity United States, 1996–2005
Clinical Manifestations- Males • Males • Can be asymptomatic • Urethritis • Epididymitis • Proctitis