Download
1 / 1
10 likes | 140 Views
Neurocognitive Impairment in HIV-Infected Subjects on HAART: Prevalence and Associations Kevin Robertson *1 , Kunling Wu 2 , Thomas Parsons 1 , Ron Ellis 3 , Marlene Smurzynski 2 , Ron Bosch 2 , Julia Wu 2 , Justin McArthur 4 , Ann C Collier 5 , Scott Evans 2 ,

E N D
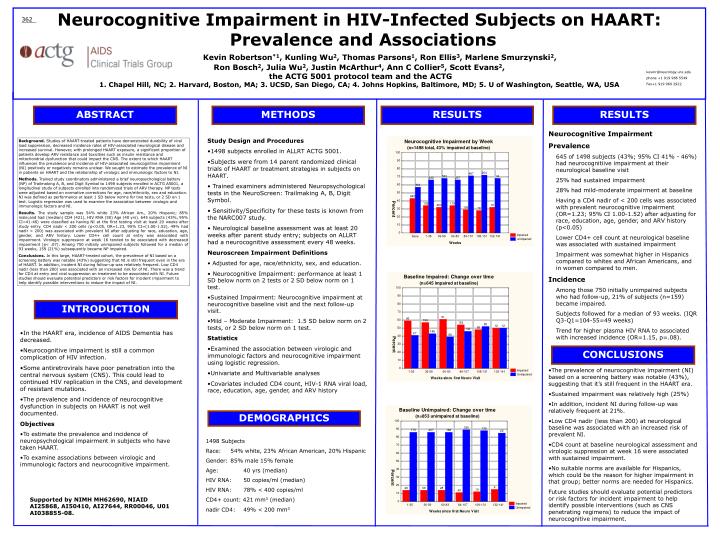
Neurocognitive Impairment in HIV-Infected Subjects on HAART: Prevalence and Associations Kevin Robertson*1, Kunling Wu2, Thomas Parsons1, Ron Ellis3, Marlene Smurzynski2, Ron Bosch2, Julia Wu2, Justin McArthur4, Ann C Collier5, Scott Evans2, the ACTG 5001 protocol team and the ACTG 1. Chapel Hill, NC; 2. Harvard, Boston, MA; 3. UCSD, San Diego, CA; 4. Johns Hopkins, Baltimore, MD; 5. U of Washington, Seattle, WA, USA 362 kevinr@neurology.unc.edu phone +1 919 966 5549 Fax+1 919 966 2922 ABSTRACT METHODS RESULTS RESULTS • Neurocognitive Impairment • Prevalence • 645 of 1498 subjects (43%; 95% CI 41% - 46%) had neurocognitiive impairment at their neurological baseline visit • 25% had sustained impairment • 28% had mild-moderate impairment at baseline • Having a CD4 nadir of < 200 cells was associated with prevalent neurocognitive impairment (OR=1.23; 95% CI 1.00-1.52) after adjusting for race, education, age, gender, and ARV history (p<0.05) • Lower CD4+ cell count at neurological baseline was associated with sustained impairment • Impairment was somewhat higher in Hispanics compared to whites and African Americans, and in women compared to men. • Incidence • Among those 750 initially unimpaired subjects who had follow-up, 21% of subjects (n=159) became impaired. • Subjects followed for a median of 93 weeks. (IQR Q3-Q1=104-55=49 weeks) • Trend for higher plasma HIV RNA to associated with increased incidence (OR=1.15, p=.08). • Study Design and Procedures • 1498 subjects enrolled in ALLRT ACTG 5001. • Subjects were from 14 parent randomized clinical trials of HAART or treatment strategies in subjects on HAART. • Trained examiners administered Neuropsychological tests in the NeuroScreen: Trailmaking A, B, Digit Symbol. • Sensitivity/Specificity for these tests is known from the NARC007 study. • Neurological baseline assessment was at least 20 weeks after parent study entry; subjects on ALLRT had a neurocognitive assessment every 48 weeks. • Neuroscreen Impairment Definitions • Adjusted for age, race/ethnicity, sex, and education. • Neurocognitive Impairment: performance at least 1 SD below norm on 2 tests or 2 SD below norm on 1 test. • Sustained Impairment: Neurocognitive impairment at neurocognitive baseline visit and the next follow-up visit. • Mild – Moderate Impairment: 1.5 SD below norm on 2 tests, or 2 SD below norm on 1 test. • Statistics • Examined the association between virologic and immunologic factors and neurocognitive impairment using logistic regression. • Univariate and Multivariable analyses • Covariates included CD4 count, HIV-1 RNA viral load, race, education, age, gender, and ARV history Background. Studies of HAART-treated patients have demonstrated durability of viral load suppression, decreased incidence rates of HIV-associated neurological disease and increased survival. However, with prolonged HAART exposure, a significant proportion of patients develop ARV resistance and toxicities such as insulin resistance and mitochondrial dysfunction that could impact the CNS. The extent to which HAART influences the prevalence and incidence of HIV-associated neurocognitive impairment (NI) positively or negatively remains unclear. We sought to estimate the prevalence of NI in patients on HAART and the relationship of virologic and immunologic factors to NI. Methods. Trained study coordinators administered a brief neuropsychological battery (NP) of Trailmaking A, B, and Digit Symbol to 1498 subjects enrolled in ACTG A5001, a longitudinal study of subjects enrolled into randomized trials of ARV therapy. NP tests were adjusted based on normative corrections for age, race/ethnicity, sex and education. NI was defined as performance at least 1 SD below norms for two tests, or 2 SD on 1 test. Logistic regression was used to examine the association between virologic and immunologic factors and NI. Results. The study sample was 54% white 23% African Am., 20% Hispanic; 85% male;and had (median) CD4 (421), HIV RNA (50) Age (40 yrs). 645 subjects (43%, 95% CI=41-46) were classified as having NI at the first testing visit at least 20 weeks after study entry. CD4 nadir < 200 cells (p<0.05, OR=1.23, 95% CI=(1.00-1.52), 49% had nadir < 200) was associated with prevalent NI after adjusting for race, education, age, gender, and ARV history. Lower CD4+ cell count at entry was associated with impairment. Virologic suppression at week 16 tended to be associated with decreased impairment (p< .07). Among 750 initially unimpaired subjects followed for a median of 93 weeks, 159 (21%) subsequently became NP impaired. Conclusions. In this large, HAART-treated cohort, the prevalence of NI based on a screening battery was notable (43%) suggesting that NI is still frequent even in the era of HAART. In addition, incident NI during follow-up was relatively frequent. Low CD4 nadir (less than 200) was associated with an increased risk for of NI. There was a trend for CD4 at entry and viral suppression on treatment to be associated with NI. Future studies should evaluate potential predictors or risk factors for incident impairment to help identify possible interventions to reduce the impact of NI. INTRODUCTION • In the HAART era, incidence of AIDS Dementia has decreased. • Neurocognitive impairment is still a common complication of HIV infection. • Some antiretrovirals have poor penetration into the central nervous system (CNS). This could lead to continued HIV replication in the CNS, and development of resistant mutations. • The prevalence and incidence of neurocognitive dysfunction in subjects on HAART is not well documented. • Objectives • To estimate the prevalence and incidence of neuropsychological impairment in subjects who have taken HAART. • To examine associations between virologic and immunologic factors and neurocognitive impairment. CONCLUSIONS • The prevalence of neurocognitive impairment (NI) based on a screening battery was notable (43%), suggesting that it’s still frequent in the HAART era. • Sustained impairment was relatively high (25%) • In addition, incident NI during follow-up was relatively frequent at 21%. • Low CD4 nadir (less than 200) at neurological baseline was associated with an increased risk of prevalent NI. • CD4 count at baseline neurological assessment and virologic suppression at week 16 were associated with sustained impairment. • No suitable norms are available for Hispanics, which could be the reason for higher impairment in that group; better norms are needed for Hispanics. • Future studies should evaluate potential predictors or risk factors for incident impairment to help identify possible interventions (such as CNS penetrating regimens) to reduce the impact of neurocognitive impairment. DEMOGRAPHICS 1498 Subjects Race: 54% white, 23% African American, 20% Hispanic Gender: 85% male 15% female Age: 40 yrs (median) HIV RNA: 50 copies/ml (median) HIV RNA: 78% < 400 copies/ml CD4+ count: 421 mm3 (median) nadir CD4: 49% < 200 mm3 Supported by NIMH MH62690, NIAID AI25868, AI50410, AI27644, RR00046, U01 AI038855-08.