Download
1 / 20
210 likes | 511 Views
INFECTIVE ENDOCARDITIS and valvular vegetations. Alex Yartsev 30/03/2010. Pathological definitions. INFECTIVE ENDOCARDITIS The colonization or invasion of heart valves or the mural endocardium by a microbe VEGETATIONS

E N D
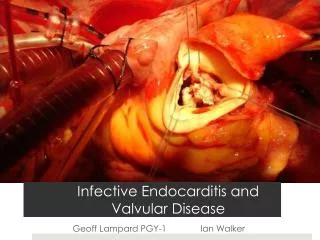
INFECTIVE ENDOCARDITISand valvular vegetations Alex Yartsev 30/03/2010
Pathological definitions INFECTIVE ENDOCARDITIS • The colonization or invasion of heart valves or the mural endocardium by a microbe VEGETATIONS • Masses of thrombotic debris and organisms, attached to valves or myocardial tissue, and destructive to that tissue Robbins and Cotran Pathologic Basis Of Disease (8th ed)
A vegetation Subacute Mitral Endocarditis, Strep viridans Acute endocarditis of congenitally bicuspid aortic valve, by Staph aureus Robbins and Cotran Pathologic Basis Of Disease (8th ed)
Acute IE or Subacute IE? • Definition dependent on virulence and course ACUTE: 10-20% of cases • Infection of a normal valve • Rapidly progressing, usually Staph Aureus • Rapidly destructive, necrotising, ulcerative SUBACUTE – 80-90% of cases • Infection of a previously diseased, deformed valve • Slowly progressing, usually Streptococcus • Gradually destructive, more like erosive Robbins and Cotran Pathologic Basis Of Disease (8th ed)
There are 3 main pathogens Defective valves: • 60% of cases its Streptococcus viridans Normal valves • Staph Aureus especially if the valve belongs to an IV drug user Prosthetic valves: • Staph epidermitis OTHER ORGANISMS: Enterococci, Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella… All oral organisms In 10-15% of cases, no organism is found. Robbins and Cotran Pathologic Basis Of Disease (8th ed)
A Word About Streptococci • Alpha hemolytic: reduce iron from hemoglobin • Strep pneumoniae, Strep viridans • Beta hemolytic: lysis of whole RBCs • Group A: S.pyogenes rheumatic fever • Group B: S.agalactiae neonatal meningitis • Group C: S.equi “distemper of horses” • Group D: Enterococci • Group G: S.canis dog saliva
Predisposing factors FOREMOST: Anything that predisposes to bacteraemia Dental procedures, oral infections,IV drug use, surgery, IV cannulas, central lines, huge obvious infections elsewhere, or minute trivial areas of slightly broken skin
Predisposing factors • Rheumatic heart disease • Mitral valve prolapse • Degenerative calcific valvular stenosis • NORMAL bicuspid aortic valve • Prosthetic valves • Unrepaired and repaired congenital defects Robbins and Cotran Pathologic Basis Of Disease (8th ed)
Complications • Brain abscess • Lung abscess • Heart failure • Glomerulonephritis (immune complexes) • Emboli anywhere
Common clinical Features • Fever, chills, rigors • New heart murmr • New onset of heart failure signs/symptoms Problems otherwise unexplained: • Brain abscesses • Lung abscesses • Glomerulonephritis
Uncommon clinical features • Roth spots (Retinal hemorrhages) • Janeway lesions (painless microabscesses ) Oslers nodes (painful immune complex deposits) Robbins and Cotran Pathologic Basis Of Disease (8th ed) Tally and O’Connor
Populations at risk • IV drug users: usually tricuspid valve • Valve replacement patients • Patients with repaired or unmanaged septal defects • Past history of rheumatic heart disease
Preventative measures • COCHRANE: “There remains no evidence about whether penicillin prophylaxis is effective or ineffective against bacterial endocarditis in people at risk who are about to undergo an invasive dental procedure. “
Diagnosis • Duke criteria: MAJOR citeria • Streptocucus viridans in blood culture • Staph aureus in blood culture in absence of primary focus • Persistently positive blood culture: organism consistent with infective endocarditis from • Blood cultures drawn more than 12 hours apart, or • all of three, or majority of four or more separate blood cultures, with the first and last drawnat least 1 hour apart • Evidence of Endocardial involvement: +ve ECHO
Diagnosis: Duke Criteria • Need 2 major • Or1 major and 3 minor • Or 5 minor criteria • MAJOR CITERIA • Positive blood culture, for a characteristic organism • Echo identification of a valvular mass or partial separation of an artificial valve
Diagnosis: Duke Criteria • MINOR CITERIA • Predisposing heart lesion • IV drug use • Vascular lesions eg. splintr hemorrhages or petechiae • Immunological phenomena eg. Oslers nodes, Roth spots • Single culture positive for an unusual organism • Echo findings consistent with but not diagnostic of endocarditis
TTE or TOE? • TTE for aortic valve • TOE for mitral, pulmonary, tricuspid • TTE less sensitive for vegetations than TOE
Practical Management • Delay of diagnosis = lower survival • Three sets of cultures before antibiotics; • Then, commence empiric therapy • Continue for 6 weeks Ohs Intensive Care Manual 6th ed; Therapeutic Guidelines
Empirical antibiotics • Therapeutic Guidelines suggest: • Benzylpenicillin 1.8 g q4h, PLUS • Flucloxacillin 2g q4h PLUS • Gentamicin 6mg/kg daily ALSO • Add Vancomycin if the pt has a prosthetic valve or the infection is hosptial-acquired
Good Evidence • COCHRANE: “There remains no evidence about whether penicillin prophylaxis is effective or ineffective against bacterial endocarditis in people at risk who are about to undergo an invasive dental procedure. “ Most people still use ampicillin or clindamycin Antibiotics for the prophylaxis of bacterial endocarditis in dentistry: Oliver et al, 2008