Download
1 / 43
450 likes | 919 Views
M.Gorky Donetsk National Medical University Department No. 2 of Pediatrics Head of the Department Dr. Churilina A.V., Ph.D. Malabsorption syndromes in children. Associated professor Masyuta D.I. Gluten-Sensitive Enteropathy (Celiac Disease).

E N D
M.Gorky Donetsk National Medical UniversityDepartment No. 2 of PediatricsHead of the Department Dr. Churilina A.V., Ph.D.Malabsorption syndromesin children Associated professor Masyuta D.I.
Gluten-Sensitive Enteropathy (Celiac Disease) • Gluten-sensitive enteropathy is a disorder in which small-bowel mucosal damage is the result of a permanent sensitivity to dietary gluten. • The disorder does not present until gluten products have been introduced into the diet. • Typically, the most common period of presentation is between 6 mo and 2 yr of age.
PATHOGENESIS • Three components interact in the pathogenesis: • toxicity of certain cereals, • genetic predisposition, and • environmental factors. • The disorder develops only after chronic dietary exposure to the protein gluten, which is found in wheat, rye, oats, and barley. • The activity of gluten resides in the gliadin fraction, which contains certain repetitious amino acid sequences (motifs) that lead to sensitization of lamina propria lymphocytes.
PATHOGENESIS • The evidence that there is a genetic predisposition is that • (1) up to 2–5% of first-degree relatives have symptomatic gluten-sensitive enteropathy, • (2) as many as 10% of first-degree relatives have asymptomatic damage to small-bowel mucosa consistent with this disorder, and • (3) there is an association of the disorder with certain human leukocyte antigen (HLA) types (B8, DR7, DR3, and DQw2).
PATHOGENESIS • Environmental factors must influence the expression of this genetic predisposition because • (1) there is a 30% rate of discordance in monozygotic twins, • (2) there is a 70% rate of discordance in HLA-identical siblings, • (3) the age of onset among siblings is variable, and • (4) the onset of symptoms can be precipitated by gastrointestinal surgery, pregnancy, antibiotic use, or a coincidental diarrheal illness.
PATHOGENESIS • The immunologic response to gluten results in • villus atrophy, • crypt hyperplasia, and • damage to the surface epithelium in the small bowel.
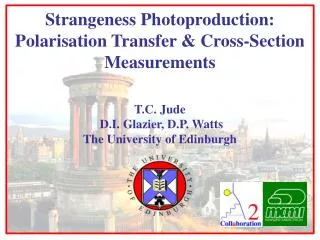
Histology of a jejunal biopsy showing lymphocytic infiltration and villous atrophy confirming coeliac disease.
PATHOGENESIS • The injury is greatest in the proximal small bowel and extends distally for a variable distance. The latter observation is undoubtedly the explanation for the variable degree of symptoms and findings of malabsorption among individuals with gluten-sensitive enteropathy. • A decrease in absorptive and digestive capacity results from a decrease in small intestinal surface area and a relative increase in immature epithelial cells. • Pancreatic secretion is decreased as a result of lowered serum cholecystokinin and secretin levels.
CLINICAL MANIFESTATIONS • The mode of presentation is variable; the majority present with diarrhea. • Children can have failure to thrive or vomiting as the only manifestation. • Perhaps as many as 10% of children referred to endocrinologists for growth retardation without an endocrine or overt gastrointestinal disorder have gluten sensitivity. • Anorexia is common and may be the major cause of weight loss or lack of weight gain.
CLINICAL MANIFESTATIONS • Infants with gluten-sensitive enteropathy are often, but not always, clingy, irritable, unhappy children who are difficult to comfort. • In contrast to infants with cystic fibrosis, they are not interested in food, although this is not always the case. • Pallor and abdominal distention are common. • Large, bulky stools have been described in some children with this condition. • Digital clubbing can occur.
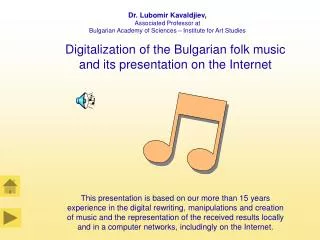
Rickets in a 3-year-old boy secondary to coeliac disease. He has frontal bossing, a Harrison's sulcus and bow legs.
Coeliac disease causing wasting of the buttocks and distended abdomen.
EVALUATION • Screening tests for malabsorption are not particularly helpful because they may be normal in a child with gluten-sensitive enteropathy. • Anemia and hypoproteinemia may be present. • The first serologic tests, including antigliadin antibodies, were not reliable enough. • However, the sensitivity and specificity of serum IgA-endomysial antibody testing have approached 100% (except in IgA-deficient patients).
EVALUATION • Histologic findings on small-bowel biopsy remain the gold standard for diagnosis and biopsy should be performed if one has a high suspicion of gluten-sensitive enteropathy or if serum endomysial antibody is found. • The strictest approach to diagnosis is to demonstrate that the biopsy returns to normal within 1–2 yr after starting a gluten-free diet and then to rechallenge with a gluten diet and repeat the biopsy. • This approach is now in evolution because it is possible to demonstrate antibody conversion while on a gluten-free diet and only an initial small-bowel biopsy may be necessary.
TREATMENT • Treatment requires a lifelong, strict gluten-free diet. • All wheat, rye, and barley products should be eliminated from the diet; many children tolerate oats. • Initially, vitamin and iron supplementation is advisable. • When the disorder presents with fulminant diarrhea, initial treatment with oral prednisone can be useful; this approach is rarely necessary.
TREATMENT • Although the parents of a child with gluten-sensitive enteropathy usually become very knowledgable about diet, initially they need the help of an experienced dietitian. • National celiac support groups provide much specific information about the gluten content of foods and medications. • Processed foods must be considered carefully because it is common that they contain some gluten. • Gluten-free foods are commercially available.
PROGNOSIS • The clinical response to a gluten-free diet of a child with celiac disease is gratifying. • Improvement of mood and appetite is followed by lessening of diarrhea. • In most cases changes occur within 1 wk of starting therapy, but the response may occasionally be delayed. • Older patients and very ill patients tend to respond slowly, but once in remission the celiac child should be treated as a well child.
Growth chart showing failure to thrive and response to a gluten-free diet.
PROGNOSIS • Subtle manifestations of growth failure or delayed sexual maturation may take place when receiving a gluten-containing diet. • Appropriately diagnosed gluten-sensitive enteropathy is a lifelong condition requiring lifelong treatment. • No complications from long-term gluten-free diet treatment are recognized.
Coeliac disease: • is a gluten-sensitive enteropathy • classical presentation is at 8-24 months with abnormal stools, failure to thrive, abdominal distension and wasted buttocks, and irritability • other modes of presentation - short stature, anaemia, screening, e.g. children with diabetes mellitus • diagnosis - positive serology (tissue transglutaminase and anti-endomysial antibodies), flat mucosa on jejunal biopsy and resolution of symptoms and catch-up growth upon gluten withdrawal • treatment - gluten-free diet for life.
Intestinal Lymphangiectasia • This group of disorders is characterized by dilatation of intestinal lymphatic vessels and leakage of lymph into the intestinal lumen and, at times, the peritoneal cavity.
Causes Of Intestinal Lymfangiectasia • Intestinal lymphangiectasia can be • primary or • can result from • abdominal or thoracic surgical damage to lymphatic vessels, • chronic right-sided heart failure, • constrictive pericarditis, • retroperitoneal tumor, or • malrotation with lymphatic obstruction.
Causes Of Intestinal Lymfangiectasia • Primary intestinal lymphangiectasia is • the result of a congenital abnormality of lymphatic drainage from the intestine and • may be associated with abnormalities in lymphatic drainage from other regions of the body. • Turner and Noonan syndromes have been associated with intestinal lymphangiectasia.
PATHOGENESIS • Because absorbed fat is normally transferred from the intestine via the lymphatic vessels, children with this disorder have steatorrhea with protein-losing enteropathy and may have lymphocyte depletion.
CLINICAL MANIFESTATIONS • Manifestations may include any combination of • hypoalbuminemia, • hypogammaglobulinemia, • edema, • lymphocytopenia, • fat malabsorption, and • chylous ascites.
Diagnosis • The diagnosis is suggested by the typical findings described previously in association with an elevated fecal alpha1-antitrypsin level consistent with protein-losing enteropathy. • The characteristic radiologic findings of uniform, symmetric thickening of mucosal folds throughout the small intestine are usually, although not always, present on small-bowel contrast radiographs.
Diagnosis • The diagnosis is confirmed by the presence of collections of abnormal dilated lacteals with distortion of villi on peroral small-bowel biopsy. • The disorder may be seen only in the submucosa, requiring surgical biopsy of the intestine.
Lactose Intolerance • Lactose intolerance is the development of clinical symptoms resulting from lactase deficiency following ingestion of lactose in water in a standard dose.
CAUSES OF LACTOSE INTOLERANCE • Primary lactose intolerance – • An autosomal recessive condition. • Results from absence of hydrolytic activity for lactose or absence of intestinal capacity to transport glucose and galactose. • Child becomes symptomatic as soon as breast or cow’s milk is started. • Responds to elimination of lactose from diet.
CAUSES OF LACTOSE INTOLERANCE • Secondary lactose intolerance – results from decreased intestinal activity secondary to damage to intestinal mucosa from some primary pathology • Acute gastroenteritis • PEM • Worm infestations • Malabsorption syndromes • Animal milk allergy • Drugs like neomycin, antimetabolites, etc.
CONSEQUENCES OF LACTOSE INTOLERANCE. • Osmotic diarrhea • Metabolic acidosis • Bacterial proliferation • Caloric loss • Pneumatosis intestinalis
CLINICAL FEATURES • Diarrhea – Watery, frothy, greenish-yellow, sour smelling stools • Perinal excoriation • Failure to thrive • Abdominal distension • Borborygmi • Flatulence
INVESTIGATIONS • Stool pH and reducing substances – • Acidic pH < 5.5 • Reducing substances > 0.5 % • Stool chromatography • Breath hydrogen test • Lactose tolerance test • Intestinal enzyme activity by biopsy
TREATMENT • Primary lactose intolerance – • Elimination of lactose from diet • Life long treatment
TREATMENT • Secondary lactose intolerance • Treatment of primary cause • Lactose free diet if • Persistent diarrhea • Weight loss • Reducing substances > 1 %