Download
1 / 43
430 likes | 666 Views
Muscle and Muscle Tissue. Chapter 9 & 10. Muscle Tissue. 3 Types Smooth – smooth muscle Skeletal – skeletal muscle Cardiac – cardiac muscle. Differ in: Structure Function Location Means of activation. Functions of Muscle. Skeletal responsible for locomotion

E N D
Muscle and Muscle Tissue Chapter 9 & 10
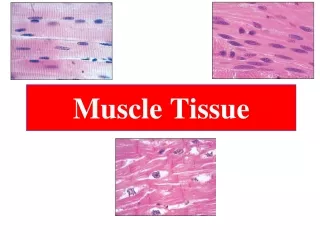
Muscle Tissue 3 Types Smooth – smooth muscle Skeletal – skeletal muscle Cardiac – cardiac muscle Differ in: Structure Function Location Means of activation
Functions of Muscle • Skeletal • responsible for locomotion • Posture, stabilize joints, generate heat • Cardiac • responsible for movement of blood • Smooth muscle • helps maintain blood pressure, and squeeze or propel substances through organs
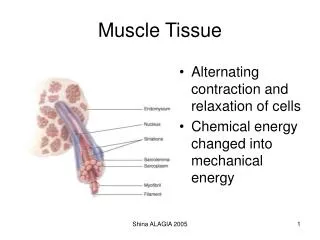
Functional Characteristics of Muscle Tissue • Excitability (irritability) – the ability to receive and respond to stimuli • Contractility – ability to shorten forcibly • Extensibility – ability to stretch or extend • Elasticity – ability to recoil and resume original resting length
Muscle Tissue Similarities Muscle Terminology Sarcolemma – muscle plasma membrane Sarcoplasm – cytoplasm of a muscle cell Prefixes: Myo Mys all mean muscle Sarco Skeletal and smooth muscle are elongated and are called muscle fibers Muscle will contract based on 2 types of microfilaments Actin Myosin
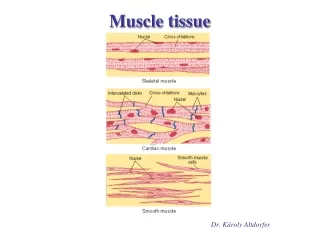
Skeletal Muscle Tissue • Muscle that attaches to and covers bone • Creates motion • Has obvious striations (stripes) • Is voluntary • most of the time • Contracts rapidly but tires easily • Extremely adaptable and can exert forces ranging from a fraction of an ounce to over 70 lbs.
Skeletal Muscle • Each muscle is an organ • Consisting of • Blood vessels • Nerve fibers • Connective tissues • Endomysium – fine sheath of connective tissue composed of reticular fibers surround each muscle fiber • Perimysium – fibrous connective tissue that surrounds a group of muscle fibers called fascicles • Epimysium – an overcoat of dense regular tissue that surrounds the entire muscle
Skeletal Muscle Nerve & Blood Supply Each muscle has One nerve One artery One or more veins Each muscle fiber has One nerve controlling contraction Muscles need Oxygen and nutrients Waste elimination Attachments Most muscles are attached to bones in 2 places Attach either Directly – epimysium of the muscle is fused to the bone Indirectly – connective tissue wrappings extend beyond the muscle as a tendon
Microscopic Anatomy • Muscle Fibers: • Each fiber is long, cylindrical with multiple nuclei just beneath sarcolemma • Each fiber has unique oxygen-binding proteins called myoglobin
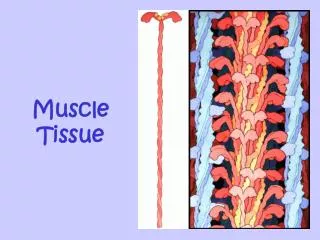
Myofibrils • Muscle fibers are made up of densely packed myofibrils • Rod like contractile elements • Myofibrils are what gives muscle its striated appearance • Because it makes perfect Dark A Bands and Light I Bands
Sarcomere • Myofibrils are composed of the sarcomeres • Smallest contractile unit of the muscle • Composed of myofilaments • Thick – myosin (entire A band) • Thin – actin (across I band and partway into A band) Z disc – connects myofibrils to one another
Sarcoplasmic Reticulum (SR) and T Tubules SR – an elaborate, smooth ER that mostly runs longitudinally and surrounds each myofibril Functions in regulation of calcium levels T Tubules – elongated tubes that penetrate the cell’s interior at the A – I band junction Conduct impulses to the deepest parts of the muscle Part of the SR
Skeletal Muscle Contraction • Sliding Filament Model of contraction: • Thin Filaments slide past Thick filaments (filaments overlap more than before) • Causes the muscle to shorten
Contraction • In order to contract a skeletal muscle must: • Be stimulated by a nerve ending – motor neurons • The size of the muscle relates to the size of the motor neuron • Receive an electrical impulse along sarcolemma and T tubules • Have a rise in Ca2+ levels (final trigger for muscle contraction)
Stages of Muscle Contraction • Cross Bridge formation – myosin cross bridge attaches to actin filament • Working (power) stroke – myosin pulls actin filament toward M line • Myosin releases actin filament • ATP attaches to myosin and the cross bridge is broken • “Cocking” of the myosin – energy for hydrolysis of ATP cocks myosin into high-energy position
Types of Contractions Isometric contraction Increasing muscle tension Muscle doesn’t shorten during contraction Isotonic Contraction Decreasing muscle length Muscle shortens during contraction
Muscle Tone • Constant, slightly contracted state of all muscles, which does not produce active movement • Keeps muscles firm, healthy, and ready to respond to stimuli
Muscle Metabolism: Anaerobic Glycolysis • When muscle contractile activity reaches 70% of the maximum • Bulging of the muscle compresses blood vessels • Oxygen delivery is impaired • Pyruvic acid is converted to lactic acid • Causes muscle soreness
Muscle Fatigue • The muscle is in a state of physiological inability to contract • Occurs when: • ATP production fails to keep pace with ATP demand • Lactic acid accumulates in the muscle
Heat Production • Only 40% of the energy released in muscle activity is actually used in the work • The remaining 60% is given off as heat
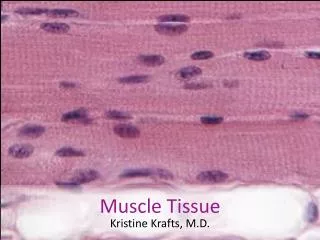
Cardiac Muscle • Found only in the heart • Striated • Involuntary • Contracts at a steady rate due to the heart’s pacemaker • Changes beat based upon body’s needs • Running – speeds up • Sleeping – slows down
Smooth Muscle • Found in the walls of hollow organs • Stomach, urinary bladder, vessels • Forces food and other substances through internal body channels • Responsible for peristalsis • Not striated • Involuntary
Smooth Muscles • Made up of small spindle –shaped fibers • Lacks the coarse connective tissue sheath of skeletal muscle • But has endomysium • Organized into 2 layers • Longitudinal – muscle fibers run parallel to the long axis of the organ • Circular – fibers run around the circumference of the organ • Has same contractile mechanism as skeletal
Peristalsis • Peristalsis – alternating contraction and relaxation of smooth muscles that mix and squeeze substances through the hollow organs • Caused by: • Longitudinal layer of smooth muscle contracts • When the longitudinal layer contracts the organ elongates
Microscopic Smooth Muscle • SR is less developed • T tubules are absent • Plasma membrane has pouch like infoldings called caveoli • No visible striations (no sarcomere)
Microscopic • Thin and Thick filaments are present • Ratio of thick to thin filaments is much lower than skeletal • Arranged diagonally – causing smooth muscle to contract in a corkscrew manner
Smooth Muscle • Some unique features of smooth muscle • Smooth muscle is very tone • Slow, prolonged contractile activity • Low energy requirements • Response to stretch
Response to Stretch • Smooth muscle exhibits a phenomenon called stress-relaxation response in which • Smooth muscle responds to stretch briefly and then adapts to new length • The new length, however, retains its ability to contract • This enables organs such as the stomach and bladder to temporarily store contents
Hyperplasia • Hyperplasia – is the ability of smooth muscle to divide and increase in number • Exhibited in women • At puberty, the estrogen stimulates the synthesis of more smooth muscle, causing the uterus to grow to adult size • At pregnancy, estrogen stimulates uterine growth to accommodate the increasing size of the growing fetus
Types of Smooth Muscle • Single Unit • Multiunit
Single Unit • Commonly called visceral muscle • Contracts rhythmically as a unit • Arranged in opposing sheets and exhibit stress-relaxation response
Multiunit • Structurally independent muscle fibers • Have a rich nerve supply • Responds to neural stimuli • Found: • Large airways to lungs • In large arteries • In arrector pilli muscle and attached to hair follicles • Internal eye muscles
Muscular Dystrophy • Muscular Dystrophy – • Group of inherited muscle destroying diseases where the muscles enlarge due to fat and connective tissue deposits, but muscle fibers atrophy and degenerate
Muscular Dystrophy • Most common type: Duchenne Muscular Dystrophy (DMD) • Inherited, sex-linked trait, carried by women and exhibited in men (1/3500) • Diagnosed between age 2-10 • Victims become clumsy and fall • Progress from extremities upward • Usually die in 20s due to respiratory failures • No cure, but myoblast therapy is promising
Developmental Aspects of Muscle • Muscle tissue develops from embryonic mesoderm called myoblast • Agrin – growth factor • Skeletal Muscle – multinucleated due to the fusing of myoblasts • Smooth and Cardiac – myoblasts do not fuse but do develop gap junctions
Regeneration • Cardiac and Skeletal muscles become amitotic but retain ability to lengthen and thicken • Satellite cells – cells that float around fixing damaged skeletal fibers • Limited regenerative ability • Cardiac cells lack satellite cells • Smooth muscle has good regenerative abilities
After Birth • Muscular development reflects neuromuscular coordination • Development occurs head-to-toe and proximal-to-distal • Athletics and training can improve neuromuscular control
Male vs. Female Men Biological factors make men stronger than women Skeletal muscle makes up 42% of body mass Men have testosterone, sex hormone due to difference in men and women Women Skeletal muscle make up 36% of body mass Body strength per unit muscle mass is about the same in males as females
Aging • With age, connective tissue increase and muscle fibers decrease • Muscles become stringier • By age 80, 50% of muscle mass is lost (sarcopenia) • Regular exercise reverses sarcopenia • Aging of cardiovascular system affects every organ in the body