Download
1 / 35
350 likes | 660 Views
Endovascular Repair of Aneurysms. Angela Diamond, MD, FACS , RVT . Endovascular Repair of Aneurysms Abdominal Aorta. Generally a disease of older males: Annual incidence of less than 1 in 1000 people younger than 60 years old Peaks at approximately 7 in 1000 people in their mid-60’s

E N D
Endovascular Repair of Aneurysms Angela Diamond, MD, FACS, RVT.
Endovascular Repair of AneurysmsAbdominal Aorta • Generally a disease of older males: • Annual incidence of less than 1 in 1000 people younger than 60 years old • Peaks at approximately 7 in 1000 people in their mid-60’s • 5 to 6 times more common in men than women.
Endovascular Repair of AneurysmsAbdominal Aorta • Risk factors include: • Male gender • Positive family history • Older age • Smoking • Coronary Artery Disease • Peripheral Vascular Disease • White race • Hypercholesterolemia.
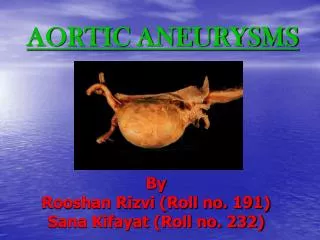
Endovascular Repair of AneurysmsAbdominal Aorta • Definition: • An aneurysm is defined as a widening or dilatation of a vessel. • The infrarenal diameter should be 1.5 times the expected diameter. • Normal diameter varies with age, sex and body weight. • Therefore, no definite diameter; however, conventionally diagnosed when the infrarenal aorta has a transverse diameter of at least 30 mm.
Endovascular Repair of AneurysmsAbdominal Aorta • The dilatation affects all 3 layers of the aorta and is usually fusiform, i.e. affecting the whole circumference. • Pathogenesis is poorly understood, the development is clearly associated with alterations in the connective tissue in the aortic wall. • The aortic wall contains vascular smooth muscle cells as well as matrix proteins - elastin and collagen.
Endovascular Repair of AneurysmsAbdominal Aorta • Histological features of an aneurysm wall: • Fragmentation of elastic fibers in the media • Dilatation of the medial wall • Then the adventia, which is primarily made up of collagen, becomes responsible for the strength of the aorta • Collagen degradation is the ultimate cause of rupture.
Endovascular Repair of AneurysmsAbdominal Aorta • The alterations in collagen and elastin in the aortic wall is dependent on production of proteases by medial smooth muscle cells, adventitial fibroblasts and the cells of the lymphomonocytic infiltrate. • Matrix Metalloproteinases (MMP’s) • Tissue Inhibitors of Matrix Metalloproteinases (TIMPs).
Endovascular Repair of AneurysmsAbdominal Aorta • Abdominal aortic aneurysms (AAA) may be asymptomatic for years; however, 30% will go on to rupture, if left untreated. • Majority of patients with ruptured aneurysms die before making it to the hospital or emergency room. • Those who make it to surgery have a high morbidity and mortality and only 10%-25% will ultimately survive until discharge.
Endovascular Repair of AneurysmsAbdominal Aorta • Risk of rupture is related to the size of the aneurysm. • Multiple studies have agreed that the risk of rupture increases to a point that elective repair is warranted when the diameter reaches 5.0 to 5.5 cm • Controversy exists in the management of small aneurysms.
Endovascular Repair of AneurysmsAbdominal Aorta • Diameter of the AAA is not the only isolated factor in risk of rupture; small aneurysms do rupture and larger ones remain stable for long periods of time. • Studies have shown that a larger initial diameter, COPD, and hypertension have all been independent predictors of rupture. • Female gender (women having a 3-fold higher risk of rupture than men), familial AAAs and smoking have also been implicated.
Endovascular Repair of AneurysmsAbdominal Aorta • Current thinking is rupture depends on diameter: • AAA < 4 cm – 0% per year, rupture • AAA 4 to 5 cm – 0.5 to 5.0 % per year, rupture • AAA 5 to 6 cm – 3 to 15 % per year, rupture • AAA 6 to 7 cm – 10 to 20 % per year, rupture • AAA 7 to 8 cm – 20 to 40 % per year, rupture.
Endovascular Repair of AneurysmsAbdominal Aorta • History and Physical Exam • Hypertension, COPD, coronary artery disease, smoking, family history of AAA. • Positive physical examination of the supra-umbilical region with bimanual palpation depends on the size of the AAA: • 61% for 3.0 to 3.9 cm • 69% for 4.0 to 4.9 cm • 82% for 5 cm or greater.
Endovascular Repair of AneurysmsAbdominal Aorta • Noninvasive Imaging: • Abdominal x-rays • Ultrasonography • Computed Tomography Angiography • Magnetic Resonance Angiography • Conventional Angiography. • US Preventive Services Task Force is now recommending screening for all men ages 65 to 75, who ever smoked, for AAA, via an abdominal aortic ultrasound.
Endovascular Repair of AneurysmsAbdominal Aorta • Medical Treatment • Beta blockers, specifically propranolol • Indomethacin • Angiotensin II blockers • Nonsteroidal anti-inflammatory drugs • Tetracyclines • HMG-CoA reductase inhibitors (statins) • Angiotensin-converting enzyme inhibitors.
Endovascular Repair of AneurysmsAbdominal Aorta • Indications for Intervention: • Rupture • > 5.5 cm • Rapid expansion in a short period of time, > 0.7cm in 6 months • Symptomatic aneurysms: patients with pain and tenderness over their aneurysm • Complications associated with aortic aneurysms: • Distal embolization • Thrombosis • Fistulization • Local compression of adjacent organs.
Endovascular Repair of AneurysmAbdominal Aorta • Open Repair: • 1923, Rudolph Matas performed the first successful aortic ligation to treat aortic aneurysm • 1930, Blakemore and King tried to induce thrombosis of the aneurysm sac by passing a current through wires that were placed into the aneurysm sac • 1940’s, cellophane was used in humans to wrap the aorta to induce periarterial fibrosis, to prevent rupture • 1951, Dubost performed the first successful aneurysm excision and repair with the use of an arterial homograft to replace an aortic aneurysm • 1954, Debakey performed an AAA repair using Dacron. In the 1950’s, aneurysms were excised prior to replacing the aorta with a graft. • 1960’s, Oscar Creech popularized the open endoaneurysmorrhaphy that we know it today, leaving the back wall of the aneurysm intact and oversewing the lumbar vessels.
Endovascular Repair of AneurysmsAbdominal Aorta • Endovascular Repair (EVAR) for an AAA was first described by Parodi et al in 1991. • This technique modeled after the work by Dotter et al was initially designed for patients too sick to undergo conventional open aortic repair. • The endograft is a vascular prosthetic graft attached to a stent and is delivered to the aorta via a transfemoral route. Under fluoroscopic guidance, the device is placed beneath the renal arteries and “deployed”- essentially relining the aorta. • Once the endograft is in place the blood travels through the device and excludes the aneurysm sac, preventing rupture. • The initial endografts were physician made.
Endovascular Repair of AneurysmsAbdominal Aorta • 3 areas of review are needed before considering the patient for an EVAR: • Proximal Neck • 1.5 cm in length, up to 32 mm in diameter • Distal Landing Zone • Ectasia and/or aneurysmal • Access Vessels • Calcium and tortuosity.
Endovascular Repair of AneurysmsAbdominal Aorta • Clinical Trial of EVAR • Endovascular Aneurysm Repair 1 Trial (EVAR-1) • Dutch Randomized Endovascular Aneurysm Management Trial (DREAM) • Open Versus Endovascular Repair Trial (OPEN) • United Kingdom EVAR Trial Investigators.
Endovascular Repair of AneurysmsAbdominal Aorta • Complications: • Endoleaks • I: Inadequate seal of proximal or distal end. • II: Flow from patent lumbar, middle sacral or inferior mesenteric artery. • III: Fabric disruption or tear. Module disconnection. • IV: Flow from fabric porosity.
Endovascular Repair of AneurysmsThoracic Aorta • The thoracic aorta can be divided into 3 segments: • The ascending aorta (from the heart to the innominate artery) • The aortic arch (from the innominate artery to the left subclavian artery) • The descending aorta (from the left subclavian artery to the level of the diaphragm) Beyond is the visceral aortic segment, wherein the renal and the visceral vessels arise.
Endovascular Repair of AneurysmsThoracic Aorta • Aneurysms of the descending thoracic aorta are mostly degenerative in nature and indistinguishable from AAA. • 20-30% of aortic aneurysm patients have a first order relative with the disease. • Continues to be a debate over whether aneurysmal degeneration is a sequela of atherosclerosis or a primary connective tissue weakness, recent studies suggest overlap.
Endovascular Repair of AneurysmsThoracic Aorta • The second most common etiology of descending thoracic aortic aneurysms is as the sequela of chronic aortic dissection. • Of patients experiencing acute aortic dissection, 25% to 40% will develop chronic aneurysmal dilatation of the outer wall of the false lumen, which renders them susceptible to late aneurysm rupture and death. • Giant cell arteritis, Marfan’s syndrome.
Endovascular Repair of AneurysmsThoracic Aorta • Expected natural history is progressive enlargement and eventual rupture, regardless of etiology or location. • Women make up half of thoracic aneurysm patients as opposed to 10%-20% of those with AAA. • Mean rate of growth for all thoracic aneurysms is 0.1 cm per year.
Endovascular Repair of AneurysmsThoracic Aorta • Natural history observations have led to the acceptance of 6 cm as the size threshold for recommendation of surgical intervention for degenerative descending thoracic aneurysms. • Or growth rates of >10 mm per year. • Increasing expansion rate is used an indicator of heightened rupture risk as is the presence of aortic tenderness, and, in some cases, consideration is given to earlier operation.
Endovascular Repair of AneurysmsThoracic Aorta Clinical presentation: • Chest and/or back pain • New onset of hoarseness • Chronic cough • Hemoptysis • Dyspnea • Dysphagia lusoria • Distal embolization. Medical treatment consists of beta blockers to keep the systolic pressure at the low normal range of 105 to 120 mm Hg, and this often requires additional medications to maintain.
Endovascular Repair of AneurysmsThoracic Aorta • Endoluminal treatment of isolated thoracic aortic aneurysms with stent grafting was introduced in 1994, by Dake et al. • Several anatomic barriers to thoracic stent grafting: • Proximal and distal seal zones should be at least 2 cm in length. • Delivery systems for thoracic endografts are larger than their abdominal counterparts, with the largest devices requiring an iliac diameter of 9 mm.
Endovascular Repair of AneurysmsThoracic Aorta • Results: • PIVITOL trial • EUROSTAR • United Kingdom Thoracic Endograft registries.
Endovascular Repair of AneurysmsPopliteal Artery • Aneurysm of >2.5 cm • If left untreated, patients do not present with rupture but with acute limb ischemia due to occlusion of the aneurysm with clot. • Stent placement via common femoral artery • Continue to need a seal zone 2 cm above and below the aneurysm, not including the tibial peroneal trunk. • Plavix and aspirin for the lifetime of the patient due to a small covered stent in a bendable part of the extremity.
Endovascular Repair of AneurysmsConclusion • Infrarenal abdominal, descending thoracic and popliteal artery aneurysms have all been successfully stented with covered stents. We do more vascular surgery stenting for aneurysms here at Harrison hospital than any other hospital in Washington state except for the University of Washington hospital system. • An aneurysm that has not been successfully stented endovascularly is a common femoral artery aneurysm due to its branching into the superficial femoral and the profunda arteries. • Thank you very much for your time today!