Download
1 / 40
480 likes | 1.05k Views
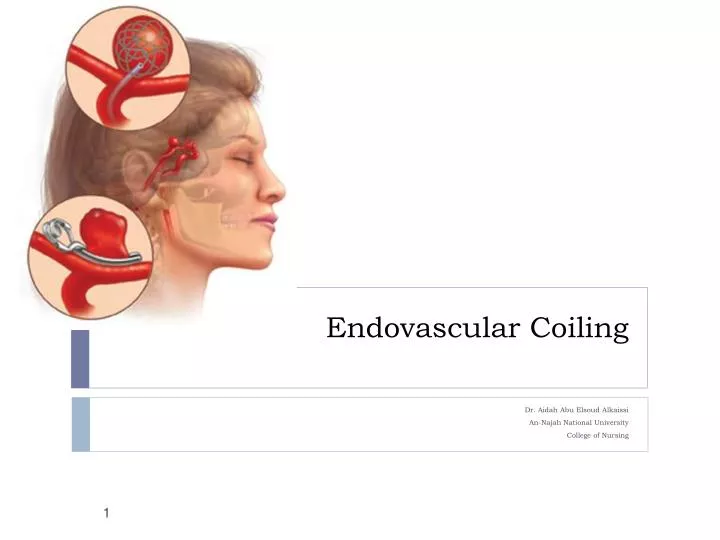
Endovascular Coiling . Dr. Aidah Abu Elsoud Alkaissi An- Najah National University College of Nursing. What is endovascular coiling?.

E N D
Endovascular Coiling Dr. Aidah Abu ElsoudAlkaissi An-Najah National University College of Nursing
What is endovascular coiling? • Endovascular coiling, also called coiling or endovascular embolization, is a procedure performed to block blood flow into an aneurysm (a weakened area in the wall of an artery). • An aneurysm in the brain may be called a cerebral aneurysm, a brain aneurysm, or an intracranial aneurysm.
Preventing blood flow into an aneurysm helps to keep the aneurysm from rupturing (bursting). Coiling does not require a surgical procedure. Rather, a catheter (a long, thin tube) is inserted into an artery in the groin, then advanced into the affected artery in the brain. X-rays are used to guide the catheter into the artery.
Coiling may also be used to treat a condition called arteriovenous malformation, or AVM. • An AVM is an abnormal connection between an artery and a vein that may occur in the brain, spinal cord, or elsewhere in the body.
The coils used in this procedure are made of soft platinum metal, and are shaped like a spring. • These coils are very small and thin, ranging in size from about twice the width of a human hair (largest) to less than one hair's width (smallest).
Aneurysms may be treated in different ways, depending on the type of aneurysm, where it is located in the brain, and the patient's medical condition. • The standard method for treating a cerebral aneurysm is called aneurysm clipping. • In this procedure, a small metal clip is used stop blood flow into the aneurysm, after an opening has been made in the skull to reach the aneurysm in the brain. • The clip looks much like a clothespin. • It is placed on the neck (opening) of the aneurysm to obstruct the flow of blood, and remains inside the brain.
Coiling is a newer procedure that has become available since the mid-1990's. • Coiling has advantages over surgical aneurysm clipping, because it does not involve opening the skull, and hospitalization time and recovery time are often shorter. • However, not everyone with a cerebral aneurysm or AVM is a suitable candidate for a coiling procedure.
Other related procedures that may be used to diagnose or treat brain disorders include cerebral arteriogram, computed tomography (CT) scan of the brain, electroencephalogram (EEG), magnetic resonance imaging (MRI) of the brain, positron emission tomography (PET) scan, x-rays of the skull, and craniotomy.
What is an aneurysm? • A cerebral aneurysm is a bulging, weakened area in the wall of an artery in the brain, resulting in an abnormal widening or ballooning. • Because there is a weakened spot in the artery wall, there is a risk for rupture (bursting) of the aneurysm.
A cerebral aneurysm generally occurs in an artery located in the front part of the brain which supplies oxygen-rich blood to the brain tissue. • A normal artery wall is made up of three layers. The aneurysm wall is thin and weak because of an abnormal loss or absence of the muscular layer of the artery wall, leaving only two layers.
The most common type of cerebral aneurysm is called a saccular, or berry, aneurysm, occurring in 90 percent of cerebral aneurysms. • This type of aneurysm looks like a "berry" with a narrow stem. More than one aneurysm may be present at the same time. • Two other types of cerebral aneurysms are fusiform and dissecting aneurysms. • A fusiform aneurysm bulges out on all sides (circumferentially). Fusiform aneurysms are generally associated with atherosclerosis.
A dissecting aneurysm may result from a tear in the inner layer of the artery wall, causing blood to leak into the layers. This may cause a ballooning out on one side of the artery wall or it may block off or obstruct blood flow through the artery. • Dissecting aneurysms may occur with traumatic injury. The shape and location of the aneurysm may affect what treatment is performed. • Most cerebral aneurysms (around 90 percent) are present without any symptoms and are small in size (less than 10 millimeters in diameter, which is less than four-tenths of an inch). Smaller aneurysms may have a lower risk of rupture.
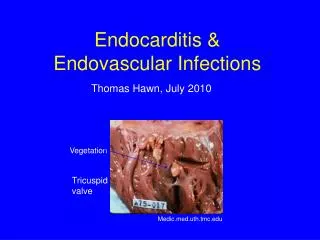
Although a cerebral aneurysm may be present without symptoms, the most common initial symptom of a cerebral saccular aneurysm is a subarachnoid hemorrhage (SAH). • SAH is bleeding into the subarachnoid space (the space between the brain and the membranes that cover the brain). • A ruptured cerebral saccular aneurysm is the most common cause (80 percent) of SAH. • SAH is a medical emergency and may be the cause of a hemorrhagic (bleeding) stroke.
Hemorrhagic strokes occur when a blood vessel that supplies the brain ruptures and bleeds. • When an artery bleeds into the brain, brain cells and tissues do not receive oxygen and nutrients. • In addition, pressure builds up in surrounding tissues, and irritation and swelling occurs. • About 20 percent of strokes are caused by hemorrhagic bleeding.
Increased risk of rupture is associated with aneurysms that are greater than 10 millimeters (less than four-tenths of an inch) in diameter, a particular location (circulation in the back portion of the brain), and/or previous rupture of another aneurysm. • A significant risk of death is associated with the rupture of a cerebral aneurysm.
How is coiling performed? • The coiling procedure may be performed by a neurosurgeon, a physician who specializes in surgery and treatment of the nervous system, and/or an interventional radiologist, a physician who specializes in diagnostic and treatments methods using radiology techniques. • Fluoroscopy (a special type of x-ray, similar to an x-ray "movie") aids in this procedure. A catheter is inserted into an artery in the groin. The catheter is guided by a small wire inside of the catheter along the length of the blood vessel to reach the area of the aneurysm. The physician uses fluoroscopy to guide the catheter to the aneurysm's location in the brain.
A microcatheter is inserted through the initial catheter. The coil is attached to the microcatheter. When the microcatheter has reached the aneurysm and has been inserted into the aneurysm, an electrical current is used to separate the coil from the catheter. The coil seals off the opening of the aneurysm. The coil is left in place permanently in the aneurysm. Depending on the size of the aneurysm, more than one coil may be needed to completely seal off the aneurysm.
Reasons for the Procedure • A coiling procedure is most commonly done to treat an unruptured cerebral aneurysm. • However, coiling may be used to treat a ruptured aneurysm in some cases. • There may be other reasons for your physician to recommend a coiling procedure.
Risks of the Procedure • If you are pregnant or suspect that you may be pregnant, you should notify your physician. • There is a risk for allergic reaction to the dye. • Patients who are allergic to or sensitive to medications, contrast media, iodine, or shellfish should notify the radiologist or technologist. • Also, patients with kidney failure or other kidney problems should notify the radiologist.
Patients who take anticoagulant (blood-thinning) medications such as aspirin, coumadin (Warfarin), clopidogrel (Plavix), or others, should notify their physician prior to the procedure, as these medications may be stopped for one or more days prior to the procedure.
Because the procedure involves the blood vessels and blood flow of the brain, there is a risk for complications involving the brain. These complications may include, but are not limited to, the following: • loss of consciousness • transient ischemic attack (TIA, a brief stroke-like condition) • hemiplegia (paralysis of one half of the body) • embolus (clot in the blood vessel) • hemorrhage (bleeding) • hematoma (an area of swelling caused by a collection of blood) • stroke • aphasia (loss of the ability or speak or the ability to understand speech) • infection • rupture of previously unruptured aneurysm
Before the Procedure- Information to the patients • Your physician will explain the procedure to you and offer you the opportunity to ask any questions that you might have about the procedure. • You will be asked to sign a consent form that gives permission to do the procedure. Read the form carefully and ask questions if something is not clear. • Notify your physician if you have ever had a reaction to any contrast dye, or if you are allergic to iodine or seafood. • Notify your physician if you are sensitive to or are allergic to any medications, latex, tape, or anesthetic agents (local and general). • You will need to fast for a certain period of time prior to the procedure. Your physician will notify you how long to fast, whether for a few hours or overnight. • Notify your physician if you are pregnant or suspect you may be pregnant.
Before the Procedure • Notify your physician of all medications (prescribed and over-the-counter) and herbal supplements that you are taking. • Notify your physician if you have a history of bleeding disorders or if you are taking any anticoagulant (blood-thinning) medications, aspirin, or other medications that affect blood clotting. It may be necessary for you to stop these medications prior to the procedure. • Your physician may request a blood test before the procedure to determine how long it takes your blood to clot. Other blood tests may be done as well. • Based upon your medical condition, your physician may request other specific preparation.
During the Procedure • A coiling procedure requires a stay in a hospital. Procedures may vary depending on your condition and your physician's practices. • This procedure is usually performed while you are asleep under general anesthesia; however, in some situations, it may be performed under local anesthesia.
Generally, a coiling procedure follows this process: • You will be asked to remove any clothing, jewelry, hairpins, dentures, or other objects that may interfere with the procedure, and will be given a hospital gown to wear. • You will be reminded to empty your bladder prior to the start of the procedure. • You will be positioned on your back on the x-ray table.
An intravenous (IV) line will be started in your hand or arm. • You will be connected to an EKG monitor that records the electrical activity of the heart and monitors the heart during the procedure using small, adhesive electrodes. Your vital signs (heart rate, blood pressure, and breathing rate) and neurological signs will be monitored during the procedure. • A catheter will be inserted into your bladder to drain urine.
The radiologist or neurosurgeon will check your pulses below the groin site where the catheter will be inserted and mark them with a marker so that the circulation to the limb below the site can be checked after the procedure. • The skin over the injection site will be cleansed. A local anesthetic will be injected.
A small incision will be made in the skin to expose the artery in the groin. • A catheter will be inserted into the artery in your groin using a guide wire. The catheter will be guided through the blood vessel into the brain using fluoroscopy. • Once the catheter has been guided to the affected artery in the brain, contrast dye will be injected to make the aneurysm and surrounding blood vessels visible on x-ray.
The aneurysm will be measured and its shape and other characteristics will be determined and recorded. • Once sufficient information about the aneurysm has been obtained, a microcatheter (smaller catheter) will be inserted into the initial catheter. A coil will be attached to the microcatheter. Fluoroscopy will be used to verify the location of the catheter inside the body.
Once the microcatheter has reached the aneurysm, the physician will manipulate the coil into the aneurysm. • When the coil has been completely inserted into the aneurysm, a small electrical current will be used to separate the coil from the catheter. • The physician will insert as many coils as needed to completely seal off the aneurysm. The coils will form a mesh-like structure inside the aneurysm. • After the aneurysm has been "packed" with coils, additional x-ray images will be taken to make sure the aneurysm has been sealed off.
Once the aneurysm has been sealed off, the catheter will be removed. To prevent bleeding, the insertion site may be closed with a device that uses collagen to seal the opening in the artery, by the use of sutures, or by applying manual pressure over the area. Your physician will determine which method is appropriate for your condition. • After the insertion site stops bleeding, a dressing will be applied. A sandbag or other heavy item such as a bag of IV fluid may be placed over the site for a period of time to prevent further bleeding or the formation of a hematoma at the site.
After the Procedure • In the hospital: • After the procedure, you may be taken to the recovery room or the intensive care unit (ICU) for observation, depending on your particular situation. • If the coiling procedure was performed for a ruptured aneurysm, you will most likely be taken to the ICU for recovery and observation. • If the coiling procedure was performed for an unruptured aneurysm and your condition is otherwise stable, you may be discharged home a day or two after the procedure.
You will remain flat in bed for as long as 12 to 24 hours after the procedure. • A nurse will monitor your vital signs, the insertion site, and circulation/sensation in the affected leg or arm. • A nurse will monitor your vital signs, your neurological signs, and the injection site while you are in the recovery room and/or the ICU. • You may be given pain medication for pain or discomfort from the procedure or from having to lie flat and still for a prolonged period. • You may resume your usual diet after the procedure, unless your physician decides otherwise.
Once you have completed the recovery period, you may be discharged to your home unless your physician decides otherwise. • In some cases after a procedure for a ruptured aneurysm, a transfer to a rehabilitation facility may be necessary to help continue recovery from damage that may have occurred as a result of the ruptured aneurysm.
At home: • You may be advised not to participate in any strenuous activities. Your physician will instruct you about when you can return to work and resume normal activities.Notify your physician to report any of the following: • fever and/or chills • increased pain, redness, swelling, or bleeding or other drainage from the insertion site • coolness, numbness and/or tingling, or other changes in the affected extremity • any changes in bodily functions or neurological changes, such as extreme headache, seizure, or loss of consciousness
Generally, a cerebral angiogram will be performed periodically after the procedure to assess the effectiveness of the coiling procedure. • The first angiogram may be performed about one month after the procedure. • Additional cerebral angiograms and/or other imaging procedures such as MR may be performed at intervals to be determined by your physician based on your condition and the results of previous post-coiling imaging procedures. • Your physician may give you additional or alternate instructions after the procedure, depending on your particular situation.