Download
1 / 28
300 likes | 624 Views
AORTIC ANEURYSMS. By Rooshan Rizvi (Roll no. 191) Sana Kifayat (Roll no. 232). Case Presentation:.

E N D
AORTIC ANEURYSMS By Rooshan Rizvi (Roll no. 191) Sana Kifayat (Roll no. 232)
Case Presentation: • A 71 year old male presented with subacute low back pain. The pain was intermittent and present for over past 1’5 months. All low back movements were also reported to be painful. The pain radiated into the posterior left leg.
On examination, blood pressure was 140/85 (controlled) and peripheral pulses were present. • No nerve root tension signs were present. Differential diagnosis: • Lumbar spinal stenosis • Lumbosacral sprain • Facet syndrome • Lumbar myofascial sprain
Radiographic examination of lumbar spine revealed extensive calcification throughout aorta and an aneurysm about its bifurcation. • At follow-up, two weeks post surgery, the low back pain had reduced to mild discomfort and leg pain had subsided.
ANEURYSM:a localized abnormal dilation of a blood vessel,or the heart
CLASSIFACATION: • Congenital or Acquired • Saccular (spherical outpouchings (involving only a portion of the vessel wall); 5 to 20 cm in diameter, often contain thrombus). or Fusiform (diffuse, circumferential dilation of a long vascular segment; diameter (up to 20 cm) )
CLASSIFICATION • True (aneurysm involves an intact attenuated arterial wall or thinned ventricular wall of the heart) e.g Atherosclerotic, syphilitic, and congenital vascular aneurysms, and ventricular aneurysms that follow transmural myocardial infarctions or False (a defect in the vascular wall leading to an extravascular hematoma that freely communicates with the intravascular space ("pulsating hematoma"). e.g a ventricular rupture after myocardial infarction that is contained by a pericardial adhesion, a leak at the sutured junction of a vascular graft with a natural artery.
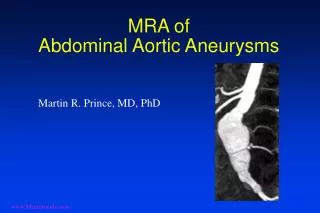
Where do aortic aneurysms tend to develop? Aortic aneurysms can develop anywhere along the length of the aorta. The majority, however, are located along the abdominal aorta. Most (about 90%) are located below the level of the renal arteries. About two-thirds of abdominal aneurysms are not limited to just the aorta but extend from the aorta into one or both of the iliac arteries.
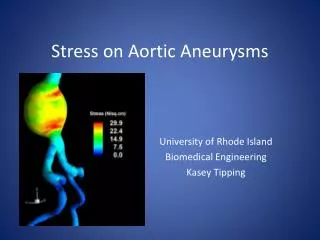
PATHOGENESIS Aneurysms occur when the structure or function of the connective tissue within the vascular wall is compromised. For example, In MARFAN SYNDROME, defective synthesis of protein fibrillin weakening of elastic tissue progressive dilaton. In EHLER-DANLOS SYNDROME, altered collagen cross-linking
PATHOGENESIS The 2 most important disorders that predispose to aortic aneurysms are • Atherosclerosis(a greater factor in abdominal aortic aneurysms), • Hypertension (most common condition associated with aneurysms of the ascending aorta) Other conditions that weaken vessel walls and lead to aneurysms include • trauma, • vasculitis, • congenital defects (e.g., berry aneurysms), and • infections (mycotic aneurysms) …..aortitis
ABDOMINAL AORTIC ANEURYSM (AAA) Aneurysms associated with atherosclerosis occur most commonly in the abdominal aorta Atherosclerotic plaque in the intima compression of the underlying media compromises nutrient and waste diffusion from the vascular lumen into the arterial wall degeneration and necrosis of the media arterial wall weakness and consequent thinning.
ABDOMINAL AORTIC ANEURYSM (AAA) Moreover, increased MMP production, especially by macrophages in atherosclerotic plaque, probably contributes to aneurysm development.
ABDOMINAL AORTIC ANEURYSM (AAA) • More frequent in men (4 times more frequent), • and smokers • Mostly after age of 50 • More common in caucasians • Frequently found in healthy older adults who are radiographed for back pain.
ABDOMINAL AORTIC ANEURYSM (AAA) Morphology: • Usually positioned below the renal arteries and above the bifurcation of the aorta • AAAs can be saccular or fusiformup to 15 cm in diameter, and up to 25 cmin length • Typically the intimal surface of the aneurysm shows severe complicated atherosclerosis with destruction and thinning of the underlying aortic media • Frequently contains a bland, laminated, poorly organized mural thrombus that may fill some or all of the dilated segment • Frequently, AAAs are accompanied by smaller aneurysms of the iliac arteries.
ABDOMINAL AORTIC ANEURYSM (AAA) Two important variants of AAA • Inflammatory AAAs are characterized by dense periaortic fibrosis containing abundant lymphoplasmacytic inflammation with many macrophages and often giant cells. …..cause is uncertain. • Mycotic AAAs are lesions that have become infected by the lodging of circulating microorganisms in the wall, particularly in bacteremia from a primary Salmonella gastroenteritis. …..suppuration further destroys the media, potentiating rapid dilation and rupture.
ABDOMINAL AORTIC ANEURYSM (AAA) • Clinical Features: • Symptoms • Commonly asymptomatic (sp small ones) • Backache • Abdominal pain • Limb claudication • May present acutely, with pain and hypotension from rupture
ABDOMINAL AORTIC ANEURYSM (AAA) • Signs: • May be palpable in abdominal aorta • Evidence of widespread vascular disease • Stigmata of distal embolization • Haemodynamic collapse with rupture
ABDOMINAL AORTIC ANEURYSM (AAA) Clinical Consequences: • Rupture into the peritoneal cavity or retroperitoneal tissues with massive, potentially fatal hemorrhage • Obstruction of a branch vessel resulting in ischemic injury of downstream tissues, for example, iliac (leg), renal (kidney), mesenteric (gastrointestinal tract), or vertebral (spinal cord) arteries • Embolism from atheroma or mural thrombus • Impingement on an adjacent structure, e.g., compression of a ureter or erosion of vertebrae • Presentation as an abdominal mass (often palpably pulsating) that simulates a tumor
ABDOMINAL AORTIC ANEURYSM (AAA) Management: In general, aneurysms of 5 cm and larger are managed aggressively, usually by surgical bypass involving prosthetic grafts. Timely surgery is critical; operative mortality for unruptured aneurysms is approximately 5%, whereas emergency surgery after rupture carries a mortality rate of more than 50%.
open AAA • surgery
THORACIC AORTIC ANEURYSMS ETIOLOGY: • most commonly associated with hypertension • Marfan syndrome • Loeys-Dietz syndromes
THORACIC AORTIC ANEURYSMS • Pathogenesis: Systemic hypertension narrowing of arterioles of the vasa vasorum outer medial ischemia "degenerative changes" of the aorta smooth muscle cell loss-or change in synthetic phenotype scarring (and loss of elastic fibers), inadequate ECM synthesis, and production of increasing amounts of amorphous ground substance (glycosaminoglycan). Histologically these changes are collectively called cystic medial degeneration
THORACIC AORTIC ANEURYSMS Signs and symptoms: • encroachment on mediastinal structures • respiratory difficulties due to encroachment on the lungs and airways • difficulty in swallowing due to compression of the esophagus • persistent cough due to irritation of or pressure on the recurrent laryngeal nerves • pain caused by erosion of bone (i.e., ribs and vertebral bodies) • cardiac disease • rupture.
THORACIC AORTIC ANEURYSMS The mortality for surgical repair of thoracic aortic aneurysms is higher than that of abdominal aneurysms. So, they are often treated conservatively unless there are signs of pregressive enlargement.