Download
1 / 36
360 likes | 376 Views
This overview covers demographics, incidence, aetiology, grading, diagnostic dilemmas, investigations, rehabilitation, outcomes, and more on spinal cord injuries. Learn about the impact, demographics, grading classifications, and diagnostic challenges associated with spinal cord injuries.

E N D
An Overview of Spinal Cord Injuries Allan Howatson ICM Clinical Fellow Teaching 11thFebruary 2016
An Overview of Spinal Cord Injuries • Demographics • Incidence and prevalence • Aetiology • Grading • Diagnostic dilemmas • Investigations • Rehabilitation • Outcomes
Litigation • Information availability • Very little accurate information on non-traumatic injury (less money involved) • Accuracy of injury severity reporting and resultant disability • It is in people’s financial interest to have more problems • Truly independent information difficult to come by • Most on-line support groups and sources of information sell advertising space to “no-win, no-fee” lawyers
Incidence and Prevalence • 1200 people paralysed per year in the UK • 1 person every 8 hours • 40,000 people living with SCI in the UK • £500 million per annum (£12,500 /person /year) • Underestimate? • Above figures only refer to those who have been through a SCI centre
Traumatic SCI • RTC – 36.8 - 50.4% • Cars > Motorbikes > Pedestrians > Cyclists • Falls – 23.8 – 41.7% • More common than RTC in the UK • Sports – 9 – 11.6% • Diving > Rugby > Horse riding > Climbing > Skiing • Assaults / Violence – 2.7 – 11.2%
Non-Traumatic SCI • Lack of data is disappointing as most series report 1/3rd of SCI’s are non-traumatic • UK = 400 people per year
Aetiology Non-Traumatic SCI • Incidence / prevalence is very difficult to determine • Published data varies widely between countries and often will exclude important causes such as “congenital”
Changes with Time • Average age of traumatic spinal cord injury is rising • 1970’s – 28.7 years old • 2003 – 37.6 years • Aetiology • Falls increasingly more common cause of SCI – most common in the >60 years old group • ? Cause of increasing mean age of SCI • Sports becoming less common cause • 14.4% in 1970’s – 9% in 2003 (USA) • Violence peaked in the 1990’s
Grading & Classifying • Terminology • Morphology • Syndromes • Spinal cord injury grading
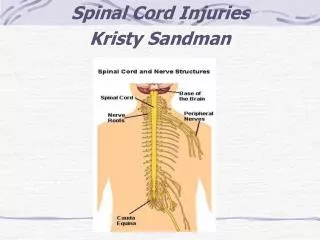
Terminology • Tetraplegia • Injury above C7/T1 resulting in loss of motor +/or sensory function • Paraplegia • Injury within thoracic, lumbar or sacral segments • Neurological level • Most caudal cord segment with normal motor and sensory function bilaterally • Usually define motor and sensory separately • Normal motor = grade 3 power with grade 5 power in all cephalad segments • Skeletal level • Vertebrae with greatest damage on imaging • Spinal shock • Flaccidity and loss of reflexes below the lesion • Neurogenic shock • Loss of sympathetic tone below the lesion
Morphology • Fracture • Fracture dislocation • SCIWORA • Penetrating
Complete and Incomplete • Complete (45% of injuries) • Absence of motor + sensory function in S5 • Zone of partial preservation • Some function below the neurological level but no function in S5 • Incomplete (55%) • S5 function preserved • Syndromes
Incomplete SCI Syndromes • Central cord syndrome • Disproportionately effects the arms compared with legs, variable sensory loss (hyperextension of the neck) • Anterior cord syndrome • Preserved dorsal column function • Brown-Sequard syndrome • Unilateral cord damage – ipsilateral loss of motor and dorsal column and contralateral loss of spino-thalamic tract function
Incomplete SCI Syndromes • Conusmedullaris syndrome • T12/L1 injury damaging lumbar and sacral segments • CaudaEquina syndrome • Injury below L1 – lower limb, bowel and bladder function loss
American Spinal Injury Association (ASIA) Grading • Complete – no motor or sensory function is preserved in the sacral segments S4–S5 • Incomplete – sensory but not motor function is preserved below the neurological level and includes the sacral segments S4–S5 • Incomplete – motor function is preserved below the neurological level, and more than half of key muscles below the neurological level have a muscle grade less than 3 • Incomplete – motor function is preserved below the neurological level, and at least half of key muscles below the neurological level have a muscle grade of 3 or more • Normal
Summarising a SCI • Skeletal level • Morphology • Cause • Resultant neurological injury • Complete / incomplete and severity • Motor and sensory neurological levels • Syndrome
Diagnostic Dilemmas • Patient assessment in the unconscious or uncooperative • The polytrauma patient • Focus on the cervical spine • SCIWORA • Investigation of other injuries in the SCI victim
Assessing the Unconscious or Uncooperative Patient • Response to pain above but not below suspected injury level • Flaccid areflexia • Flexed elbows – unable to extend • See-saw respiration in the absence of airway obstruction/chest injury • Inappropriate vasodilatation • Bradycardia in the face of hypotension • Hypotension un-response to fluid • Priapism • Loss of anal tone/reflexes
The Polytrauma Patient • Spinal injuries and therefore potential cord injuries go hand in hand with major trauma • Blunt polytrauma: 1-10% cervical spine injury • 2-10% of those with head injury have cervical spine injury • 25% of those with a cervical spine injury have a head injury • 20-60% of those with traumatic spinal cord injury will significant other injuries too
Our Focus on the Cervical Spine • Justified! • 55% of spinal injuries are in the cervical spine (15% thoracic, 15% T-L junction, 15% lumbosacral) • Cervical spine injuries are the potentially most devastating if missed • But… • 10% of those with cervical spine injury have a second spinal injury elsewhere
SCIWORA • Spinal Cord Injury Without Radiological Abnormality • SCIWO - ionising radiation demonstrating an - A • Rare with the advent of MRI • Still used as a label by some clinicians even if MRI demonstrates a lesion
Other Injuries in those with SCI • Must look very closely • Loss of sensation of pain masks other injuries • Spinal shock will result in the loss of helpful clinical signs (guarding)
Investigations in Suspected SCI • Clinical • NEXUS • Canadian C-spine Rule (CCR) • Imaging • Plain radiograph • CT • MRI
Clinical Clearance of the C-Spine • NEXUS • National Emergency X-Radiography Utilization Study • No posterior midline cervical-spine tenderness • No evidence of intoxication • Alcohol, drugs • Analgesia • A normal level of alertness (GCS 15) • No focal neurologic deficit • No painful distracting injuries
Imaging • Plain radiographs • 3 traditional views • Base of skull to C7/T1 junction • Miss 5-10% of injuries in the unconscious patient • CT • Base of skull to T4, AP and lateral views of T and L spines (or re-construct T and L spine from CT) • MRI • Details cord injury • Particularly of use in those with non-traumatic injury
Outcomes • >90% survive the injury • SCI increases mortality risk • Higher neurological level • Complete SCI • Older age • Older date of injury • Best predictions made at 72 hours post injury • Complete SCI – expect one motor level improvement • Incomplete SCI – 50% chance of walking
Rehabilitation • 12/13/14 spinal cord injury centres in the UK & Ireland • Multi-disiplinary • A lot of complete SCI rehabilitation is focused on living with a deficit rather than improving one • Home alterations, wheelchairs, psychological support etc. • Much more improvement expected from those with incomplete injury • 21% never go home • 20% depressed
Summary • SCI are a major burden on the economy • The mechanisms of injury and the people suffering them are changing • Good quality information on non-traumatic SCI is lacking • Classification and summarising SCI • Investigation of suspected SCI • Living with a spinal cord injury
References • Papers • Ho CH, Wuermser LA, Priebe MM, Chiodo AE, Scelza WM, Kirshblum SC. Spinal cord injury medicine. 1. Epidemiology and classification. Arch Phys Med Rehabil 2007;88(3 Suppl 1):S49-54 • IG Stiell, CM Clement, RD McKnight, et al. The Canadian C-Spine Rule versus the NEXUS Low-Risk Criteria in Patients with Trauma. N Engl J Med 2003; 349: 2510-8 • McKinley WO, See1 RT, Hardman JT. Nontraumatic spinal cord injury: incidence, epidemiology, and functional outcome. Arch Phys Med Rehabil1999;80:619-23. • JW McDonald, C Sadowsky. Spinal-cord injury. Lancet 2002; 359: 417–25 • JS Harrop, S Naroji, MG Maltenfort et al. Neurologic Improvement After Thoracic, Thoracolumbar, and Lumbar Spinal Cord (ConusMedullaris) Injuries. SpineVol 36, No. 1, pp 21–25 • P Rouleau, E Ayoub, PA Guertin. Traumatic and Non-Traumatic Spinal Cord-Injured Patients in Quebec, Canada: 1. Epidemiological, Clinical and Functional Characteristics. The Open Epidemiology Journal, 2011, 4, 133-139 • KL Vanderhave, Schiravuri, MS Cairdet al. Cervical Spine Trauma in Children and Adults: Perioperative Considerations. J Am AcadOrthopSurg2011;19:319-327 • PAC Lim, AM Tow. Recovery and Regeneration after Spinal Cord Injury: A Review and Summary of Recent Literature. Ann Acad Med Singapore 2007;36:49-57 • CH Ho, LA Wuermser, MM Priebe et al. Spinal Cord Injury Medicine. 1. Epidemiology and Classification. Spinal Cord Injury Medicine. 2. Acute Care Management of Traumatic and NontraumaticInjury. Spinal Cord Injury Medicine. 3. Rehabilitation Phase After Acute Spinal Cord InjuryArch Phys Med RehabilVol88, Suppl1, March 2007 • Websites • http://www.apparelyzed.com/statistics.html • https://www.nscisc.uab.edu/ • http://www.trauma.org • Texts • ATLS Manual • Oh’s Intensive Care Manual • Oxford Desk Reference: Critical Care