Download
1 / 11
110 likes | 249 Views
Mental practice in chronic stroke- results of a randomized, placebo-controlled trial. Background& purpose. Mental practice (MP) = motor imagery Similarity between MP and physical practice Neural and muscular structures activation Time taken to mentally and physically perform movement

E N D
Mental practice in chronic stroke- results of a randomized, placebo-controlled trial
Background& purpose • Mental practice (MP) = motor imagery • Similarity between MP and physical practice • Neural and muscular structures activation • Time taken to mentally and physically perform movement • Speed accuracy tradeoff is maintained • Autonomic events • Addition of MP rather than conventional motor therapy only is better for both subacute and acute stroke p’t
Hypothesis • MP group would show significantly greater fine motor function changes • MP+ physical practice group would exhibited lager score increase on the Fugl-Meyer impairment score
Method Outcome measures: • 66-point, upper extremity section of the Fugl-Meyer assessment of motor recovery after stroke (FM) • Action research arm test (ARA): grasp, grip pinch, and gross movement
Method Participants • Volunteers recruited by advertisement posted in neurological and physical clinics. Inclusion: • No more than one stroke • Able to flex at least 10∘ from neutral at the affected wrist and MP and IP joints • Stroke experience > 12 months • score≥69 on the MMSE • Age > 18 and <80 years
Method Exclusion: • Excessively spasticity (MAS≥3) • Excessive pain (VAS≥4) • Still in any form of rehab. • Participating in any experiment
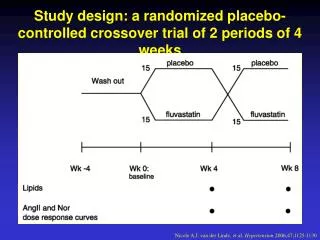
Method • Single-blinded, multiple baseline, randomized, pre- and post-test control group • 2 days per week, 30 min segments for 6 weeks • One week after therapy completion, each subject returned to the laboratory to do the post-test R+PP 30-minute tape of progressive relaxation program MP+PP 30-minute tape of mental practice
Result • The group did not differ significantly on any of the interval level baseline measures, which were age, time poststroke, FM score, and ARA score. • ARA: MP+PP improved average of 7.81 points R+PP improved average of 0.44 points • FM: MP+PP improved mean of 6.72 points R+PP improved mean of 1 point
Discussion • MP is thought to render its impact by at least 2 independent but interrelated mechanism • Increase affected arm use • Use-dependent brain reorganization new cortical areas are recruited to assist in the movement of the affected arm. • First randomized controlled, appropriately powered support to the hypothesis.
Limitation • Did not use objective measures of affected arm use, such as activity monitors • Did not use neuroimaging to confirm the neural mechanism of the treatment effect • Measurement of the duration of the MP effect
Conclusion • Traditional rehab. + mental practice during therapy increases outcomes significantly.