Download
1 / 39
390 likes | 921 Views
DOUBLE BLIND DOUBLE DUMMY PLACEBO CONTROLLED RANDOMIZED CLINCAL TRIAL OF IMPLANTABLE NALTREXONE (PRODETOXONE) FOR HEROIN ADDICTION. Evgeny Krupitsky, MD, PhD, D.Med.Sci. St.-Petersburg Bekheterv Research Psychoneurological Institute and St.-Petersburg Pavlov State Medical University.

E N D
DOUBLE BLIND DOUBLE DUMMY PLACEBO CONTROLLED RANDOMIZED CLINCAL TRIAL OF IMPLANTABLE NALTREXONE (PRODETOXONE) FOR HEROIN ADDICTION Evgeny Krupitsky, MD, PhD, D.Med.Sci. St.-Petersburg Bekheterv Research Psychoneurological Institute andSt.-Petersburg Pavlov State Medical University
CONFLICT OF INTERESTS • Supported withNIDA grant R01-DA-017317 • Dr. Krupitsky has received funding as a consultant for Alkermes, Inc.
PHARAMCOTHERAPY OF HEROIN DEPENDENCE • Full agonists (methadone, LAAM) • Partical agonists-antagonists (buprenorphin) • Full antagonists (naltrexone, nalmefene)
NALTREXONE Different drug formulations: 1. Oral 2. Implantable 3. Injectable
Background Our previous studies with oral naltrexone demonstrated its superiority over placebo, however, the rate of abstinence was relatively low in six month of medication (Krupitsky et al, J. Substance Abuse Treatment, 2002, 23:273-283) • Combination of oral naltrexone with antidepressants improved abstinence insignificantly (Krupitsky et al, J. Substance Abuse Treatment, 2006, 31:319-328)
The major problem with oral naltrexone is a poor compliance Is there way to improve naltrexone therapy ?
DIFFICULTY WITH ORAL NTXN: POOR COMPLIANCE “The pessimist sees difficulty in every opportunity. The optimist sees opportunity in every difficulty” Winston Churchill OPPORTUNITY: EXTENDED RELEASE FORMULATIONS
Implantable Naltrexone: Route and Dosage PRODETOXONE, tablets for implantation1000 mg of naltrexone
Pharmacokinetics of Prodetoxone(data from the manufacturer) Concentration, ng/ml 0 10 20 30 40 50 60 70 Time after implantation, days Naltrexone metabolite Naltrexone Blood samples were collected in one week, one and two months after implantation
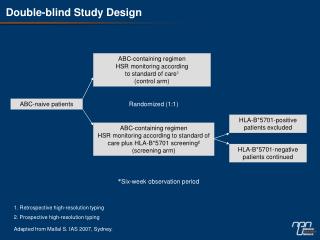
METHODS • 306 male and female heroin addicts after detoxification, giving informed consent and passing a Naloxone challenge had been randomly assigned to one of three treatment groups (102 PATIENTS EACH). Three cell study design:1. Naltrexone Implant (1000 mg) (3 times, every 2 months) + Oral Placebo (OP+NI). 2. Oral Naltrexone (50mg/day) + Implant Placebo (3 times, every 2 months)(ON+PI).3. Implant Placebo(3 times, every 2 months)+ Oral Placebo (OP+PI). • All patients received biweekly clinical management / compliance enhancement counseling. • Treatment lasted 6 months. • Control of abstinence, compliance, psychiatric symptoms, and side effects – every other week. • All patients had at least one family member who was able to supervise medication compliance. • Study design: Double blind double dummy placebo controlled randomized clinical trial.
Assessments • Assessments have been done at baseline, at each biweekly appointment, and at 3 and 6 months following the end of treatment. • Assessments included: Psychiatric rating scales, Riboflavine control of compliance, Urine drug tests, Naloxone challenge. • Primary outcomes: Treatment retention and relapse to heroin dependence. • Secondary outcomes: Opiate negative urines, HIV risk, psychiatric symptoms, and other measures of adjustment.
Recruitment details 358 approached 309 met inclusion criteria 306 got randomized
Retention in treatment (Remission) (% of patients) + + + * * + * * * P<0.01 to placebo + * * + + P<0.01 to ON+PI + + * + * * + + * * * + + + * + + * * * * + * * + * * + * * * * * Weeks
Kaplan-Meier Survival Functions: Drop out Log Rank (Mantel-Cox) Sig. P(NI+OP)- (PO+PI)<0,001 P(NI+OP)- (PI+ON) <0,001 P(ON+PI)- (PO+PI)=0,069
Retention: End of treatmernt(6 months) OP+NI > OP+PI (P<0,001) OP+NI > ON+PI (P<0,001) (P<0,001) (P<0,001)
Remissions in 3 & 6 months after treatment * (3 Month Follow Up) (6 Month Follow Up) (End of Treatment) *Follow ups collected for 46,5% of those who was randomized
Opiate negative visits P<0,001 * * * * * P<0,001 * * * * * * * P<0,001 *- P<0,01 Fisher's Exact Test to placebo + - P<0,01 Fisher's Exact Test to Ntxn implant group
Genetic AnalysisThomas Kosten, MDDavid Nielsen, PhDBaylor College of Medicine I). Gens of µ-opiate receptors: • OPRM11, 2) OPRM12, 3) OPRM13 II). Gene of κ-opiate receptor: OPRK1 III). Gene of the enzyme COMT: COMT
[OPRM13,COMT,OPRK1] 0,6 [AAAGTT] or [AGAGTT] the others 0,5 0,4 0,3 0,2 0,1 0,0 PO/NI (p=0.9) ON/PI (p=0.056) PO/PI (p=0.031) Effect of genotype on the completion of the treatment: Uncertainty Coefficients (I)
[OPRM11,COMT,OPRK1] 0,6 [CCAGTT] or [CTAGTT] the others 0,5 0,4 0,3 0,2 0,1 0 PO/NI (p=0.89) ON/PI (p=0.075) PO/PI (p=0.056) Effect of genotype on the completion of the treatment: UncertaintyCoefficients (II)
Effect of genotype on the completion of the treatment: Kaplan-Meier Survival Functions (p=0.03) (p=0.02)
Effect of genotype on the completion of the treatment: Treatment Effectiveness Score p=0.043 p=0.063
Use of other drugs Fisher's Exact Test P=0,005 to placebo Fisher's Exact Test P=0,049 to ON+PI
Anxiety and Depression State Anxiety (Spielberger scale) Depression (Beck scale)
Anhedonia (Chapmanat al.) Physical Anhedonia Social Anhedonia
Anhedonia (J. Ferguson et al.) LACK OF PLEASURE LACK OF INTEREST
HIV Risk Assessement Battery RAB drug risk RAB sex risk
AE(non-surgical) (% visits) AE (surgical) (% implants) POP+IP=0.005 PON+IP=0.0001
Most common AE Abdominal discomfort Nausea Drowsiness None of them required any special medication. Two patients in NI+OP group were terminated from the study because of side effects (wound infection).
SAE The was only one serious adverse event in PI+OP group – the holecystectomia due to the stones in gallbladder which was considered as probably not related to the study medication
OD at the follow-up Through the phone calls to patients or their relatives follow-up information was collected on 261 patient (85,3% of the study patients). According to this information, five patients died during the 12 month follow-up period, all of them died of overdose, four of them were in the PI+OP (double placebo) group and one – the PI+ON group.
Summary • Implantable naltrexone demonstrated greater effectiveness in the treatment of heroin dependence in comparison to oral naltrexone and placebo. • Implantable naltrexone is basically comparable to oral naltrexone and placebo in terms of safety and tolerability except surgical adverse events. • Genotyping is helpful to determine responders to treatment.
LIMITATIONS for PRODETOXONE • Surgical procedure • Wound infections (particularly in HIV+ individuals) • Cosmetic defects • Relatively easy to take out within the first few weeks after implantation • Dos not provide 2 months long blockade in some patients (small proportion)
AKNOWLEDGEMNET E. Zvartau, E. Blokhina, V. Egorova, D. Masalov, А. Burakov, М. Tsoy, N. Bushara, Т. Romanova, Е. Verbitskaya, A. Tyurina, V. Palatkin, Ch. О’Brian, G. Woody,T. Kosten, D. Nielsen St.-Petersburg Pavlov State Medical University,St.-Petersburg Bekheterev Research Psychoneurological Institute, University of Pennsylvania, Baylor College of Medicine Supported withNIDA grant R01-DA-017317