Download
1 / 21
220 likes | 446 Views
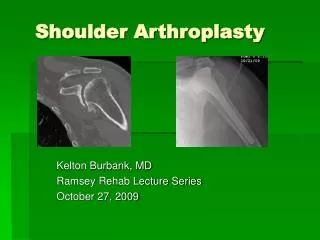
The Shoulder & Pectoral Girdle (2). Imaging. X-ray shows sublaxation, dislocation, narrow joint space, bone erosion, calcification in soft tissues Arthrography detecting rotator cuff tears, Bankart lesions found with anterior stability. Imaging.

E N D
Imaging • X-ray shows sublaxation, dislocation, narrow joint space, bone erosion, calcification in soft tissuesArthrography detecting rotator cuff tears, Bankart lesions found with anterior stability
Imaging • CT scan cuff tears + labral detachmentsUltrasound rotator cuff tearsMRI rotator cuff pathology – instability- osteonecrosis of head of humerus- staging of tumors Arthroscopy intra articular lesions- detachments of the labrum- capsule & impingement or tears of the rotator cuff
Adhesive Capsulitis • Characterized by progressive pain and stiffnessIt usually resolves after about 18 months The causes remain unknown
Clinical features • The patient, age 40-60 years may give a history of trauma, followed by aching in the arm and shoulderPain gradually increase in severity prevent sleeping on the affected sideStiffness becomes an increasing problemA frozen shoulder looks quite normal + some wastingNot much tenderness markedThere is lack of activity and passive movements in all directions
Diagnosis • When patient is seen exclude: infection, post-traumatic stiffness, diffuse stiffness and reflex dystrophy
Calcification of the Rotator Cuff ( Acute Calcific Tendinitis) • Acute shoulder pain may follow deposition of calcium in the supraspinatus tendon The cause is unknown
Clinical features • The condition affects 30-50 year olds following overuse The pain subsides after few daysDuring acute stage, the arm is held immobileCalcification is seen just above the greater tuberosity on an x-ray
Rupture of Long Head of Biceps • Patient always over 50 yearsWhile lifting, the patient feels something snap in the shoulder & upper arm becomes painful and bruised Ask the patient to flex the elbow, you’ll see a prominent lump in lower part of the arm
Impingement Syndrome • Arises from repetitive compressing or rubbing of the rotator cuff tendons (mainly supraspinatus) under the coracoacromial archIf arm is abducted and then externally and internally rotated as in cleaning a window, the rotator cuff may be compressed as it comes in contact with the acromion process & coracoacromial ligament Impingement position ( abduction, slight flexion, internal rotation)
Instability of the Shoulder • If the humeral head is not held in place, recurrent dislocation or recurrent sublaxationIn 95% of cases the displacement is anteriorIt can also be posterior or multidirectional
Anterior Instability • It follows acute injury in which the arm is forced into abduction, external rotation, and extension
Posterior Instability • The condition is due to a violent jerk in an unusual positionRecurrent posterior instability usually takes the form of sublaxation when the arm is used in flexion and internal rotation
Multidirectional Instability • The condition is associated with capsular and ligamintous laxity, and sometimes with weakness of the shoulder muscleLittle force is required to displace the jointMuscle strengthening and training in joint control are helpful
Habitual Sublaxation • Dislocation can occur more or less spontaneously if there are congenital anatomical abnormalities or sever ligamintous laxityThe patient can voluntarily sublaxate or dislocate the shoulder, painlessly and reduce it again easily
Tuberculosis • Constant ache & stiffness lasting many monthsWasting of muscles around the shoulder especially the deltoid
Rheumatoid Arthritis • The most common joint disease to affect the shoulderAcromioclavicular erosion discovered on an x0ray of the chest is the first clue of the diagnosis
Osteoarthritis • Patient is usually aged 50-60 years There is a restriction in shoulder movement in all directionsArticular space may be narrowed + osteophyte formation + bone sclerosis
Arthroplasty • The process of replacing the joint with an artificial joint
Arthrodesis • Indications : Paralysis of the scapulohumeral musclesInfective disorders of the glenohumeral jointAdvanced erosive arthritis with massive disruption of the rotator cuff