Download
1 / 20
200 likes | 333 Views
Neuromodule Approach to Pain. Melzack's Gate Theory is revolutionary, helpful, but wrong. Some people experience pain without ANY injury. Doesn’t explain injury-less pain, such as Quinlan Phantom limb pain Pain occurs only because of CNS activity—neuromodules.

E N D
Neuromodule Approach to Pain Melzack's Gate Theory is revolutionary, helpful, but wrong. Some people experience pain without ANY injury. Doesn’t explain injury-less pain, such as Quinlan Phantom limb pain Pain occurs only because of CNS activity—neuromodules. Neuromodules are like software programs, or tracks on CDs Should be triggered by major event (i.e., serious injury) but for some people are trigged by minor event (i.e., bad mood).
Neuromodule Approach to Pain Fred. Lenz: Locates brain cells panic attacks. Smell and memory Emotions launched via peripheral activity: Bite that pencil! Neuromodules may explain "pain epidemics” Neuromodule confirmed by new pain killers that reduce brain excitability. Anti-epileptic drugs Sea snail venom ABT-594—from frogs. 70X more powerful than morphine. Take home point: Pain is "all in the head"
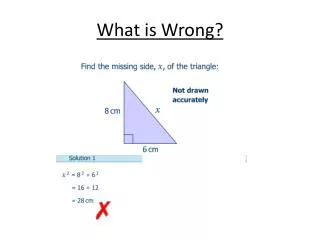
Early Trauma and Increased Pain Sensitivity • 1. Infant rats have paw injected with irritant, or not. • 2. Mature rats exposed to hot surface: • * To injured paw • * To uninjured paw • * "Control" rats • 3. Injured rats respond quicker, but only for hurt paw • 4. Injured rats have more pain-nerve endings • 5. Implications for humans: • * Surgery w/o anesthesia • * Treatment of premature infants
Neuromodule Model Memories of previous injuries Emotions YOWW!! Injury to Periphery
Phantom Limb Pain I placed a coffee cup in front of John and asked him to grab it. Just as he said he was reaching out, I yanked the cup away. "Ow!" he yelled. "Don't do that!" "What's the matter?" "Don't do that," he repeated. "I had just got my fingers around the cup handle when you pulled it. That really hurts!" Hold on a minute. I wrench a real cup from phantom fingers and the person yells, ouch! The fingers were illusory, but the pain was real - indeed, so intense that I dared not repeat the experiment. V.S. Ramachandran Phantoms in the Brain Phantom limbs will: Itch, twitch, gesticulate during conversation, and will take actions “on their own”. Phantom limb paralysis: Brain “learns” that attempts to move missing limb fail, translate it into paralysis, creates excruciating cramps.
Alleviating Phantom Limb Pain 1. Patient places healthy limb and stump into mirror box. 2. Look through top, at angle, “see” two limbs. 3. Move healthy limb in “mirror symmetric movement”, like orchestra conductor or clapping hands. 4. Creates artificial visual feedback of phantom limb being intentionally controlled. 5. Patient then instructed to clench good hand, tightly—sees both hands clenched. 6. Patient told to slowly unclench “both hands”, and phantom limb relaxes, providing relief to chronic pain. 7. Repeated trials led one patient to “loose” phantom arm, but phantom hand now attached to shoulder! Mirror Box
Phantom Limb Patient Using Mirror Box Ramachandran, Phantoms in the Brain Philip rotated his body, shifting his shoulder, to "insert" his lifeless phantom into the box. Then he put his right hand on the other side of the mirror and attempted to make synchronous movements. As he gazed into the mirror, he gasped and then cried out, "Oh, my God! Oh, my God, doctor! This is unbelievable. It's mind boggling!" He was jumping up and down like a kid. "My left arm is plugged in again. It's as if I'm in the past. All these memories from so many years ago are flooding back into my mind. I can move my arm again. I can feel my elbow moving, my wrist moving. It's all moving again. V. Ramachandran
Can Healthy Limbs Be “Fooled”? (From Ramachandran) 1. Purchase a realistic but fake arm/hand - Sit at table with one hand resting on the table, the other beneath the table. - Position the fake arm/hand on the table in the corresponding position as though both hands/arms are resting on the table. - Have associate tap both real hand that is beneath table and the fake hand in synchrony as you watch the fake hand. - Notice how sensations appear to originate from the fake hand/arm. 2. Carry out the same on naïve associate. - Once the effect has been achieved for a while, pull out previously hidden hammer and hit the fake arm/hand. - Run!
Musings on Responses to Others’ Pain Why ”oooohhhhh!!!!”? Why is others’ pain funny?
Types of Chronic Pain a. Benign pain 1. Lasts for at least 6 mos. 2. Non-responsive to Tx 3. Example: lower back pain b. Recurrent acute pain 1. Repeated episodes of sharp, acute pain, with pain free periods in between. 2. Last for at least 6 mos. 3. Example: Migraine headaches. c. Chronic progressive pain 1. Duration: at least 6 mos. 2. Increases in severity over time 3. Example: Cancer, degenerate diseases
Life Meaning of Chronic Pain You are in car accident, suffer chronic back pain that severely reduces your freedom of movement. What areas of your life would be affected? Emotional toll: Depression Work / Independence Social / interpersonal implications Leisure activities Income / Standard of Living Declined ability to deal with other life stresses
Psycho-social Complications of Chronic Pain • 1. Counterproductive coping • a. Isolation • b. Negative beliefs • 2. Social Support: • a. Hazards of positive support • b. Hazards of no support • Negative stereotypes • Medical complications and risks • 5. Double binds (1-4, above)
Pain Prone Personality Are some personalities more prone to experiencing, reporting pain? MMPI = Minnesota Multiphasic Personality Inventory a. Acute pain pats: Hypochondriasis – overly attend to body Hysteria – extreme emotionality/exaggerate symps. b. Chronic pain pats: Neurotic triad: Hypcondriasis + hysteria + depression Secondary gain: What are social benefits of pain? Attention, special identity “Functional type”: neurotic triad + schizo / psychopathology / paranoia Danger of “Pain Prone Personality” concept? 1. Negative stereotypes 2. Causal direction
Pain and Depression Wrong model: Pain Depression --- What’s missing? Correct model: Pain ↓ activity ↓ mastery ↓ control Depression
“MECHANICAL” PAIN REDUCTION TECHNIQUES Drugs Surgery Sensory Control: Counter-irritation Counter-irritation stim. Dorsal horn cells inhibit pain-transit cells.
“PSYCHOSOCIAL” PAIN REDUCTION TECHNIQUES Biofeedback Relaxation Hypnosis Acupuncture Distraction Guided Imagery Cognitive Reframing Pain Management Programs
Pain Relief Through Virtual Reality Severe burns one of most painful conditions to treat: cleaning, re-bandaging excruciating. Pennebaker symptom research suggests that distraction should do what to pain? Reduce it. Why? Competition of cues. SnowWorld: Virtual Reality program designed for pain relief. Patients enter SnowWorld during procedures Shoot snowballs at snowmen, penguins Report pain reductions 30%-50% Note SnowWorld colors. Why?
Pain Management Programs 1. Evaluation a. pain b. functional status: life style changes, limitations c. Emotional and mental functioning 2. Treatment plan a. Pre-set time. Not indefinite. b. Specific goals. c. Contract 3. Program a. Education 1. Nature of pain: physio, psychological 2. Pain reduction techniques b. Therapy 1. Psycho therapy 2. Cognitive therapy: c. Family therapy d. Relapse prevention