Download
1 / 33
340 likes | 488 Views
Refractory Hypertension: Four Cases. Paul R. Chelminski, MD, MPH, FACP Associate Professor of Medicine Associate Residency Program Director. Objectives. 1.Review JNC-7 Guidelines 2.Understand common barriers to achieving blood pressure control

E N D
Refractory Hypertension:Four Cases Paul R. Chelminski, MD, MPH, FACP Associate Professor of Medicine Associate Residency Program Director
Objectives 1.Review JNC-7 Guidelines 2.Understand common barriers to achieving blood pressure control 3.Review some causes of secondary hypertension. 4.Review recent advances in our understanding of the HTN management
JNC-7* Highlights • CVD risk doubles with each 20/10mmHg increment over 115/75 • SBP more important CV risk factor • Two or more agents usually required • Thiazides are first choice and first line • Consider 2 agents if BP >20/10 above goal • Targets • 140/90 • 130/80 if diabetic or CKD *Joint National Committee on the Prevention, Detection, Evaluation and Treatment of High Blood Pressure, 7th Report http://www.nhlbi.nih.gov/guidelines/hypertension/express.pdf.
HTN Control: Clinical Impact • Decreased CVD Incidence • Stroke:35-40% • MI: 20-25% • CHF: >50% • 12mmHg BP reduction over 10 yrs will prevent one death in every 11 patients • NNT is 9 patients with underlying CVD or target organ damage
BP Control in Clinical Settings • >70% non-diabetic & diabetic patients with sub-optimal control • 91% adherent to regimens • 70% taking fewer than 3 antihypertensives • “Therapeutic Inertia”: • 45% did not have therapy intensified at first f/u visit • 36% had no change at 2nd f/u visit
Challenges to Improving Blood Pressure Control Four Cases of Refractory Hypertension
Barriers to HTN control Cost Medication side effects Lack of gratifying response to therapy (patient does not feel better) Need for lifestyle changes Tedium: titration- requiring multiple visits & close monitoring by MD & patient
Case 1 Visit 1 • 61 yo female with HTN, hyperparathyroidism, h/o DVT • Presents with “pins & needles” in LE’s • Meds • coumadin, Sensipar • amlodipine, lisinopril, furosemide, HCTZ, metoprolol • Social Hx: non-smoker,uninsured • BP 194/129 (re-check, 172/111); ?non-adherence to one medication; recent SBP’s ~140 • Labs: Na 145, K 3.7, Cr 0.8, Ca 11.7, B12 465 • Dispo: Restart meds & f/u 4 days
Case 1 Visit 2 • c/o Fatigue • Patient confirms medications • BP 204/132 (re-check, 210/135) • Receives clonidine in clinic & admitted for hypertensive urgency & management of hypercalcemia
Case 1 Hospitalization & Visit 3 • Hydrated with decrease in Ca++ • Source of HTN identified: non-adherence d/t inability to afford meds • D/C Meds: lisinopril, metoprolol, furosemide (Walmart $4drugs to rescue) • BP at f/u 147/101 • Amlodipine added
Obstacles to Optimizing HTN Management • Adherence • Cost • Literacy! • Clinical Uncertainty • 50% doctors don’t intervene due to uncertainty about accuracy of triage BP (home blood pressures lower) • Competing Medical Demands • Trial evidence conflicting about influence of multiple comorbididities • Time constraints • Largely unstudied
Case 2 • 54 yo female with HTN, diabetes, hypercholesterolemia • BP Meds: amlodipine, lisinopril, HCTZ spironolactone • BP 7/09: 166/83; A1c 9.0%: Substitute chlorthalidone for HCTZ • BP 1/09: 164/68; A1c: 7.3%: ?Non-adherence to one med
Case 2 • Social Hx: No tobacco; no ETOH; h/o cocaine use but denies current.
Drugs That Cause HTN • Drugs of abuse • Cocaine, methamphetamine • Alcohol • OTC decongestants • Prescription • Venlafaxine/SNRIs • Estrogens/OCP’s • Corticosteroids • Namenda • Erythropoietin • Tacrolimus/Cyclosporin
Case 3 • 62 yo male with HTN, palpitations, myalgias • Meds: felodipine (5mg), atenolol (100mg), benazepril (20mg), minoxidil (10mg prn elevated BP), KCL 80mEq/d • Social: no tobacco; retired farmer • ROS: no CP, no SOB/DOE, no syncope • BP 182/99, P 64. +S4 gallop • Labs: K+ 2.8; aldo 90, renin <0.2 (ratio=450)
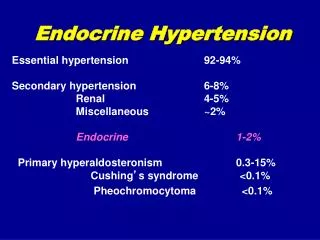
Case 3 • Dx: Hyperaldosteronism • Etiology: Adrenal adenoma (rare malignancy), adrenal hyperplasia • W/U: • Aldo/Renin: Ratio >30 suggests primary hyperaldosteronism • MRI of abdomen • Rx • Medical: spironolactone • ?Surgery
Case 3: Denouement • Spironolactone, 100mg bid started • Orthostasis at home with SBP’s in 70’s • Decreased minoxidil to 5mg/d and atenolol to 50mg/d • BP 139/90 • K+ (4.7)-palpitations, myalgias resolved.
Case 4 • 77yo female with refractory HTN, diet controlled DM, obesity, OA
Case 4 • BP 159/79 (Re-check, 160/79) • ROS: Daytime sleepiness, snoring, night-time arousals • K+ 4.1, Cr 0.87 • Sleep study: OSA • Denouement: Awaiting outcome of CPAP trial
Study objective Comparison of cardiovascular events between group treated with combination benazepril-HCTZ versus combination benazepril-amlodipine, with hypothesis that benazepril-amlodipine would be superior in reducing cardiovascular events. HCTZ
Study design Total 11,506 patients recruited for study Multi-center Randomized, double-blind trial Similar patient demographic and co-morbidities in each group Intention to treat model
Who are the patients? This study has a high predominance of patients who are elderly, obese, Caucasian, have multiple co-morbidities (including diabetes, dyslipidemia, and CAD), and difficult to control HTN, requiring multiple agents. “at high risk for cardiac events”
Who are the patients? • 38% Receiving 3 or more drugs at enrolment • Only 37% had BP <140/70 • 60% had diabetes • Average age 68yrs (fairly geriatric)
Study procedures (cont’d) Algorithm outlined by study for optimization of blood pressure control
Study Endpoints Primary endpoint Time to first event One event per patient Composite of a cardiovascular event and death from cardiovascular causes Secondary endpoints Multiple events counted for a patient Including composite of cardiovascular events, hospitalization from heart failure, death from any cause
Results: Improved BP Control Both benazepril/ amlodipine and benazepril/ HCTZ combination therapy improved blood pressure control
Results: CV Mortality and Events Benazepril/amlodipine group saw: Decreased primary endpoints at 30 mos. Decrease secondary endpoints: death from CV causes, non-fatal MI< stroke Early cessation of study by safety & monitoring committee when pre-specified thresholds for termination seen in Ace/CCB arm d/t efficacy
Drug Costs Adapted from Blue Cross Blue Shield of North Carolina and WalMart $4 pharmacy list 90 supply available from Drugstore.com for $18